-
 ⚡️ Reduced Price ⚡️ Take advantage ⚡️ Reduced Price ⚡️ Take advantage
⚡️ Reduced Price ⚡️ Take advantage ⚡️ Reduced Price ⚡️ Take advantage -
-
-
-





Anti-Alcohol Protector - 90 capsules
Anti-Alcohol Protector - 90 capsules
Couldn't load pickup availability
Share
La fórmula Protector Anti-Alcohol de Nootrópicos Perú integra complejo sinérgico de fitoquímicos bioactivos, precursores de glutatión y cofactores vitamínicos en formas optimizadas, diseñado para respaldar capacidad metabólica hepática de procesamiento de acetaldehído mediante soporte a sistemas de detoxificación de fase I y fase II, favoreciendo homeostasis redox celular y función de enzimas aldehído deshidrogenasa y alcohol deshidrogenasa que catalizan oxidación secuencial de etanol. Esta formulación contribuye a mantenimiento de integridad mitocondrial durante estrés oxidativo asociado con metabolismo de alcohol, proporciona soporte a ciclo de urea mediante provisión de ornitina que participa en conversión de amonio, y favorece neutralización de especies reactivas generadas durante oxidación de etanol en hepatocitos mediante precursores de sistemas antioxidantes endógenos.
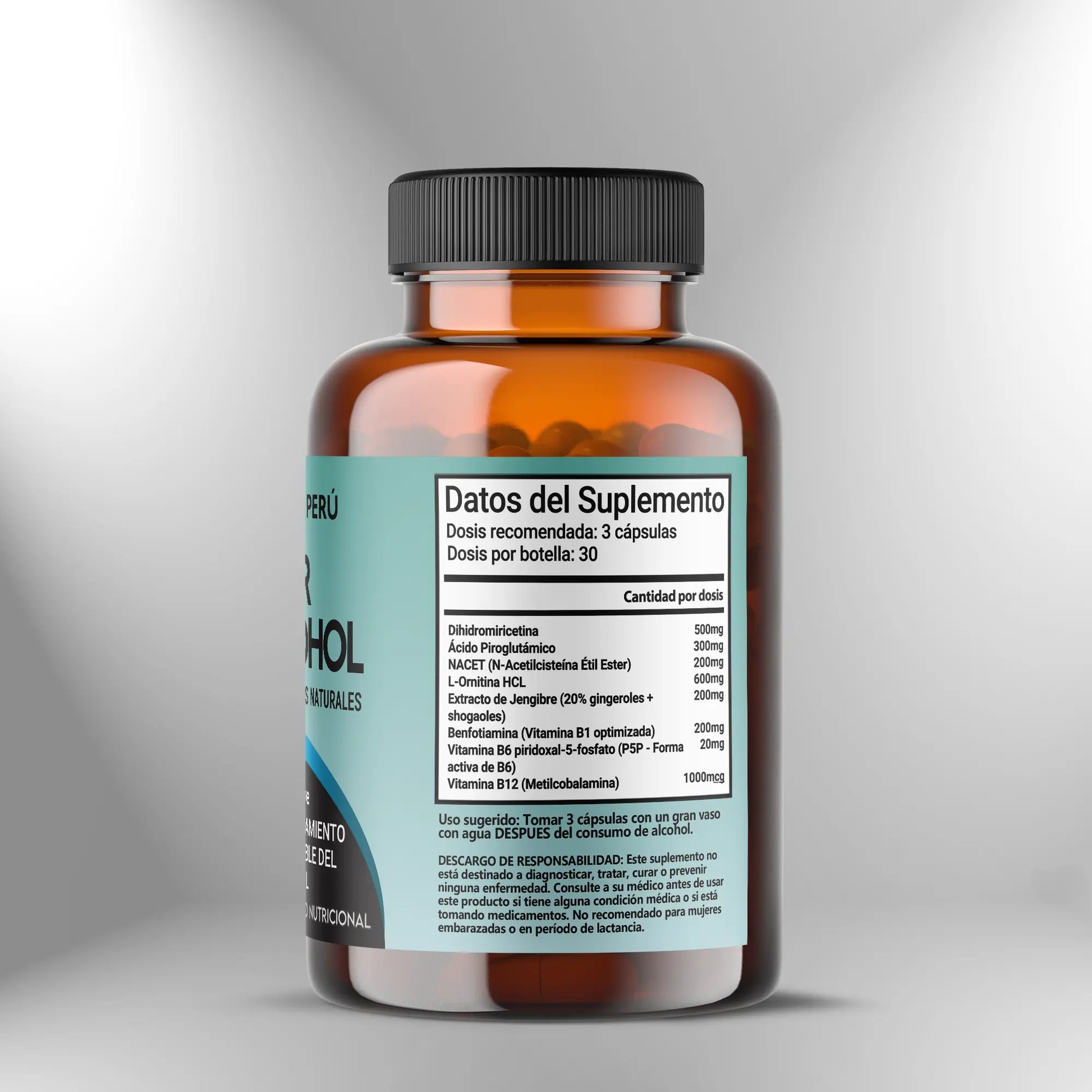
Dosis preventiva - 2 a 3 cápsulas
Para uso preventivo antes de consumo de alcohol, administre dos a tres cápsulas aproximadamente treinta a sesenta minutos antes de iniciar ingesta de bebidas alcohólicas, permitiendo tiempo para absorción intestinal de componentes y distribución a tejidos incluyendo hígado donde metabolismo de etanol ocurre predominantemente. La administración preventiva favorece que cofactores vitamínicos estén disponibles en forma activa cuando enzimas que los requieren son activadas durante metabolismo de alcohol, que precursores de glutatión estén presentes en hepatocitos antes de que consumo de glutatión sea incrementado durante conjugación de acetaldehído, y que compuestos moduladores de enzimas de detoxificación como dihidromiricetina y extracto de jengibre estén en circulación sistémica cuando exposición a alcohol comienza. La dosis de dos cápsulas puede ser apropiada para consumo moderado de alcohol definido como una a dos bebidas estándar durante periodo de dos a cuatro horas, mientras tres cápsulas pueden ser más apropiadas para consumo más extenso o cuando la duración de exposición a alcohol se extiende durante varias horas. La efectividad de dosificación preventiva depende de timing apropiado donde administración muy temprana puede resultar en metabolismo y eliminación de componentes antes de que exposición a alcohol ocurra, mientras administración durante o después de consumo de alcohol puede no permitir establecimiento de niveles tisulares óptimos de cofactores y precursores antes de que demanda metabólica sea incrementada.
Dosis de soporte activo - 2 a 3 cápsulas
Durante consumo activo de alcohol que se extiende durante varias horas, puede administrarse dosis adicional de dos a tres cápsulas aproximadamente dos a tres horas después de dosis preventiva inicial para mantener niveles circulantes de componentes que son metabolizados y eliminados durante periodo de exposición prolongada. Esta estrategia de dosificación escalonada es particularmente relevante para componentes con vida media relativamente corta incluyendo NACET que es hidrolizado por esterasas y metabolizado rápidamente, y vitaminas hidrosolubles del complejo B que son excretadas en orina cuando concentraciones plasmáticas exceden capacidad de reabsorción tubular renal. La administración durante consumo de alcohol debe realizarse con alimentos o al menos con líquidos abundantes para facilitar deglución y dilución gástrica, reduciendo probabilidad de molestia gástrica que puede ser incrementada cuando alcohol y suplementos concentrados están presentes simultáneamente en estómago. Evite exceder dosis total de seis cápsulas en periodo de veinticuatro horas para prevenir ingesta excesiva de componentes individuales particularmente vitaminas del complejo B donde límites superiores tolerables aunque elevados para la mayoría de vitaminas B establecen techo de seguridad, y para mantener exposición a componentes bioactivos dentro de rangos estudiados. La decisión de administrar dosis de soporte activo debe basarse en duración y cantidad anticipada de consumo de alcohol, donde eventos sociales breves con consumo limitado pueden no requerir dosificación escalonada mientras eventos extensos con consumo sostenido pueden beneficiarse de mantenimiento de niveles de componentes mediante administración adicional.
Dosis post-consumo - 2 a 3 cápsulas
Tras finalizar consumo de alcohol, administre dos a tres cápsulas antes de acostamiento o tan pronto como sea práctico después de último consumo de bebida alcohólica, favoreciendo que procesamiento de alcohol residual que continúa durante horas subsecuentes a consumo ocurra en contexto de disponibilidad optimizada de cofactores y precursores. La administración post-consumo es crítica dado que metabolismo de alcohol continúa mientras etanol y acetaldehído están presentes en circulación y tejidos, proceso que puede extenderse durante seis a ocho horas después de consumo dependiendo de cantidad ingerida y tasa metabólica individual que varía sustancialmente entre personas debido a polimorfismos en genes que codifican alcohol deshidrogenasa y aldehído deshidrogenasa. Durante periodo nocturno mientras sueño ocurre, hígado continúa procesando alcohol mediante oxidación que genera acetaldehído y especies reactivas que consumen glutatión y generan estrés oxidativo, haciendo que provisión de precursores de glutatión mediante NACET y cofactores para enzimas de detoxificación durante este periodo respalda procesamiento continuo sin interrupción por depleción de sustratos o cofactores. La administración con alimento ligero o al menos con agua abundante es recomendable para facilitar absorción y reducir probabilidad de molestia gástrica, aunque algunos individuos toleran administración sin alimentos particularmente si sensibilidad gástrica no es problemática. Asegure hidratación apropiada consumiendo al menos dos a tres vasos de agua con dosis post-consumo y antes de acostamiento, dado que alcohol tiene efectos diuréticos mediante inhibición de hormona antidiurética que incrementa pérdidas urinarias de líquidos, y deshidratación contribuye a manifestaciones adversas asociadas con consumo de alcohol mediante múltiples mecanismos incluyendo concentración incrementada de metabolitos en sangre y tejidos, y compromiso de perfusión cerebral.
Uso como soporte metabólico hepático regular - 2 cápsulas diarias
Para personas que consumen alcohol regularmente con frecuencia de tres o más días semanales, la administración de dos cápsulas diarias con comida principal independientemente de timing de consumo de alcohol proporciona soporte continuo a capacidad de detoxificación hepática y homeostasis redox, favoreciendo mantenimiento de reservas de glutatión, expresión apropiada de enzimas de detoxificación, y función mitocondrial en hepatocitos que pueden ser comprometidas durante exposición crónica a alcohol. Esta aproximación de dosificación basal es distinta de dosificación preventiva aguda donde dosis es sincronizada con evento específico de consumo de alcohol, y en lugar establece provisión sostenida de cofactores y precursores que optimiza status basal de sistemas de detoxificación permitiendo que respondan más efectivamente a episodios de exposición a alcohol. La administración con comida que contiene proteínas y grasas favorece absorción de componentes lipofílicos y quelados, y reduce probabilidad de molestia gástrica que puede ocurrir con administración en ayunas particularmente durante uso prolongado. Implemente ciclos de uso de ocho a doce semanas de administración diaria seguidos de pausas de siete a diez días que permiten evaluación de función hepática basal sin suplementación activa y previenen dependencia de provisión exógena de precursores que podría teóricamente downregular síntesis endógena aunque evidencia de este fenómeno con componentes en esta fórmula es limitada. Durante pausas, mantenga alimentación equilibrada rica en proteínas de alta calidad que proporcionan aminoácidos azufrados incluyendo cisteína y metionina que son precursores endógenos de glutatión, vegetales crucíferos que contienen compuestos azufrados que inducen expresión de enzimas de fase II, y fuentes de vitaminas del complejo B incluyendo granos enteros, legumbres y productos animales.
Timing estratégico y consideraciones de absorción
La absorción y biodisponibilidad de componentes en esta fórmula son moduladas por presencia de alimentos, estado de acidez gástrica, y timing en relación a consumo de otras sustancias que pueden interferir con absorción o metabolismo. La administración con alimentos que contienen grasas favorece absorción de benfotiamina que es derivado lipofílico de tiamina, y puede moderar velocidad de absorción de componentes hidrosolubles reduciendo concentración pico pero extendiendo duración de absorción estableciendo perfil farmacocinético más sostenido. Sin embargo, para uso preventivo donde objetivo es alcanzar niveles circulantes elevados rápidamente antes de exposición a alcohol, administración sin alimentos o con alimento muy ligero puede ser preferible para maximizar velocidad de absorción. El NACET como éster lipofílico de N-acetilcisteína tiene biodisponibilidad mejorada comparado con N-acetilcisteína y no requiere estómago vacío para absorción apropiada, aunque algunos individuos experimentan náusea leve con administración en ayunas particularmente en dosis elevadas. Evite consumo simultáneo con antiácidos o inhibidores de bomba de protones que neutralizan o reducen acidez gástrica, dado que ambiente ácido facilita desintegración de cápsulas y solubilización de algunos componentes, aunque impacto sobre absorción de componentes en formas optimizadas es menor comparado con sales simples que requieren ionización en ambiente ácido. Mantenga separación de al menos dos horas entre esta fórmula y suplementos de minerales en dosis elevadas particularmente calcio, magnesio o zinc que pueden formar complejos con componentes reduciendo absorción, y suplementos de fibra en dosis muy elevadas que pueden adsorber componentes en lumen intestinal reduciendo contacto con mucosa para absorción.
Ajustes según patrón de consumo de alcohol y respuesta individual
La dosificación óptima varía sustancialmente entre individuos dependiendo de múltiples factores incluyendo cantidad y frecuencia de consumo de alcohol, tasa metabólica individual determinada por polimorfismos genéticos en enzimas que metabolizan alcohol y componentes de fórmula, masa corporal que determina volumen de distribución, y sensibilidad individual a manifestaciones asociadas con consumo de alcohol. Para individuos con masa corporal elevada superior a noventa kilogramos o con consumo de alcohol en cantidades que exceden tres a cuatro bebidas estándar, considere incremento de dosis preventiva a tres cápsulas y dosis post-consumo a tres cápsulas para proporcionar cofactores y precursores en cantidades proporcionalmente mayores que compensan volumen de distribución incrementado y carga metabólica elevada. Para personas con sensibilidad gástrica conocida o historial de intolerancia a suplementos, inicie con una cápsula durante primer uso evaluando tolerancia digestiva, y progrese a dosis estándar de dos a tres cápsulas solo si tolerancia es apropiada sin manifestaciones de náusea, malestar epigástrico o cambios en evacuaciones. Si experimenta molestia gástrica con dosis estándar, administre con alimento sustancial que proporciona matriz que amortigua contacto directo con mucosa, divida dosis total en dos administraciones espaciadas temporalmente, o reduzca a dos cápsulas si tres generan manifestaciones. Los individuos que metabolizan alcohol rápidamente debido a variantes genéticas de alcohol deshidrogenasa con actividad incrementada pueden experimentar acumulación acelerada de acetaldehído requiriendo énfasis en componentes que favorecen actividad de aldehído deshidrogenasa incluyendo vitaminas del complejo B, mientras metabolizadores lentos pueden beneficiarse más de componentes que modulan alcohol deshidrogenasa como dihidromiricetina. Mantenga registro de dosis utilizada, timing de administración, cantidad de alcohol consumida y respuesta percibida que proporciona retroalimentación para optimización de protocolo individual mediante ajustes iterativos basados en experiencia acumulada.
Integración con estrategias de reducción de impacto de alcohol
La suplementación con Protector Anti-Alcohol debe integrarse como componente de aproximación integral a minimización de efectos adversos asociados con consumo de alcohol que incluye estrategias conductuales y nutricionales complementarias. Consuma alimentos antes y durante ingesta de alcohol, priorizando alimentos que contienen proteínas, grasas saludables y carbohidratos complejos que enlentecen absorción de alcohol reduciendo velocidad de incremento en concentración sanguínea de etanol y permitiendo que metabolismo hepático procese alcohol más efectivamente sin saturación completa de capacidad enzimática. Mantenga hidratación apropiada alternando bebidas alcohólicas con agua en ratio de uno a uno minimizando deshidratación que contribuye a manifestaciones adversas, y consumiendo al menos dos a tres vasos de agua antes de acostamiento y al despertar para facilitar eliminación de metabolitos y rehidratación. Limite consumo de alcohol a cantidades moderadas evitando consumo excesivo que satura capacidad de detoxificación hepática independientemente de suplementación, generando acumulación de acetaldehído y estrés oxidativo que excede capacidad de protección. Evite mezclar diferentes tipos de bebidas alcohólicas que pueden contener congéneres que son compuestos adicionales generados durante fermentación incluyendo metanol, acetona, taninos y aldehídos que contribuyen a efectos adversos y requieren detoxificación adicional. Priorice sueño de calidad y duración apropiada tras consumo de alcohol reconociendo que aunque alcohol puede facilitar inicio de sueño, compromete arquitectura de sueño reduciendo sueño REM y sueño profundo que son fases críticas para recuperación, estableciendo déficit de sueño que contribuye a manifestaciones al día siguiente. Consuma desayuno equilibrado rico en proteínas, frutas y vegetales al día siguiente que proporciona aminoácidos para regeneración de proteínas hepáticas, antioxidantes dietéticos que complementan sistemas endógenos, y carbohidratos que restauran glucógeno hepático depletado durante metabolismo de alcohol que inhibe gluconeogénesis.
Dihidromiricetina (DHM)
La dihidromiricetina es flavonoide extraído de Hovenia dulcis que modula actividad de alcohol deshidrogenasa y aldehído deshidrogenasa, enzimas que catalizan oxidación secuencial de etanol a acetaldehído y acetaldehído a acetato respectivamente, favoreciendo metabolismo eficiente de alcohol y reduciendo acumulación de acetaldehído que es metabolito altamente reactivo. La DHM también modula receptores GABA-A en sistema nervioso central mediante mecanismo que contrarresta efectos de etanol sobre estos receptores, contribuyendo a homeostasis de neurotransmisión. Estudios preclínicos sugieren que DHM puede favorecer protección hepática durante exposición a etanol mediante modulación de estrés oxidativo y expresión de enzimas de detoxificación, aunque mecanismos moleculares precisos continúan siendo caracterizados. La biodisponibilidad de DHM es moderada con metabolismo hepático significativo, haciendo que dosis y timing de administración sean consideraciones importantes para optimización de efectos.
Ácido piroglutámico
El ácido piroglutámico, también llamado pidolato o 5-oxoprolina, es derivado cíclico de ácido glutámico que participa en ciclo gamma-glutamil como intermediario en metabolismo de glutatión. Durante síntesis y degradación de glutatión, ácido piroglutámico es generado mediante ciclización de glutamato terminal de glutatión por gamma-glutamil ciclotransferasa, y es convertido de vuelta a glutamato por 5-oxoprolinasa utilizando ATP. El ácido piroglutámico puede modular homeostasis de glutatión mediante efectos sobre disponibilidad de glutamato que es precursor limitante para síntesis de glutatión cuando cisteína y glicina están disponibles. La provisión de ácido piroglutámico puede favorecer mantenimiento de pools de glutatión durante periodos de demanda incrementada como metabolismo de acetaldehído que consume glutatión mediante conjugación catalizada por glutatión S-transferasas. El ácido piroglutámico también puede actuar como osmolito orgánico modulando volumen celular y puede influir en función cognitiva mediante mecanismos que incluyen modulación de neurotransmisión colinérgica, aunque evidencia en contexto de exposición a alcohol es limitada.
NACET (N-acetilcisteína etil éster)
El NACET es derivado lipofílico de N-acetilcisteína donde grupo carboxilo es esterificado con etanol, incrementando lipofilicidad que favorece permeabilidad a través de membranas celulares y barrera hematoencefálica comparado con N-acetilcisteína que tiene permeabilidad limitada debido a carga negativa de grupo carboxilo. Una vez dentro de células, ésteres son hidrolizados por esterasas liberando N-acetilcisteína que proporciona cisteína biodisponible para síntesis de glutatión, tripéptido compuesto de glutamato, cisteína y glicina que actúa como antioxidante endógeno más importante y como cofactor de glutatión peroxidasas y glutatión S-transferasas. El metabolismo de acetaldehído consume glutatión mediante conjugación que genera aductos glutatión-acetaldehído que son excretados, y mediante neutralización de especies reactivas de oxígeno generadas durante metabolismo oxidativo de alcohol, haciendo que provisión de precursores de glutatión es relevante durante exposición a etanol. El NACET también puede modular inflamación mediante efectos sobre NF-kappaB que regula expresión de genes proinflamatorios, y puede favorecer función mitocondrial mediante mantenimiento de homeostasis redox que protege complejos respiratorios de daño oxidativo.
L-ornitina HCl
La L-ornitina es aminoácido no proteinogénico que participa en ciclo de urea, vía metabólica hepática que convierte amonio tóxico generado durante catabolismo de aminoácidos en urea que es excretada por riñón. Durante metabolismo de alcohol, generación de acetaldehído y su oxidación a acetato incrementan producción de NADH que inhibe gluconeogénesis y favorece catabolismo de aminoácidos incrementando generación de amonio, haciendo que ciclo de urea opera a capacidad incrementada. La ornitina es sustrato de ornitina transcarbamilase que cataliza condensación de ornitina con carbamil fosfato formando citrulina, primer paso comprometido de ciclo de urea que ocurre en mitocondrias hepáticas. La provisión de ornitina puede favorecer capacidad de ciclo de urea de procesar amonio particularmente durante periodos de generación incrementada, aunque efectividad depende de disponibilidad de carbamil fosfato y función apropiada de enzimas subsecuentes del ciclo. La ornitina también puede modular secreción de hormona de crecimiento y poliaminas que participan en proliferación celular y reparación tisular, aunque relevancia de estos efectos en contexto de exposición a alcohol requiere caracterización adicional.
Extracto de jengibre (20% gingeroles + shogaoles)
El extracto de jengibre estandarizado contiene gingeroles y shogaoles que son compuestos fenólicos picantes responsables de propiedades bioactivas de Zingiber officinale. Los gingeroles modulan inflamación mediante inhibición de ciclooxigenasas y lipooxigenasas que catalizan síntesis de prostaglandinas y leucotrienos proinflamatorios, y mediante inhibición de NF-kappaB que regula expresión de genes que codifican citoquinas incluyendo TNF-alfa e IL-6. Durante metabolismo de alcohol, generación de acetaldehído y especies reactivas de oxígeno activa vías de señalización inflamatoria en hepatocitos y células de Kupffer que son macrófagos residentes en hígado, contribuyendo a estrés hepático. Los compuestos del jengibre también modulan motilidad gastrointestinal mediante efectos sobre receptores serotoninérgicos y colinérgicos que regulan peristalsis y vaciamiento gástrico, favoreciendo función digestiva que puede ser comprometida durante exposición a alcohol. Los shogaoles que son productos de deshidratación de gingeroles durante procesamiento o almacenamiento exhiben potencia incrementada en algunos ensayos de actividad antiinflamatoria y antioxidante. El extracto de jengibre también modula metabolismo de xenobióticos mediante efectos sobre expresión de enzimas de fase II incluyendo glutatión S-transferasas que conjugan acetaldehído y otros electrófilos facilitando eliminación.
Benfotiamina (vitamina B1 optimizada)
La benfotiamina es derivado lipofílico sintético de tiamina donde grupo hidroxilo en posición 4 del anillo pirimidina es sustituido con grupo S-acil, incrementando lipofilicidad que favorece absorción intestinal y permeabilidad celular comparado con tiamina hidrocloruro que tiene biodisponibilidad limitada. Una vez absorbida, benfotiamina es desfosforilada por fosfatasas intestinales y hepáticas liberando tiamina que es fosforilada intracelularmente formando tiamina pirofosfato que es forma coenzimática activa. La tiamina pirofosfato es cofactor de enzimas que participan en metabolismo de carbohidratos incluyendo piruvato deshidrogenasa que convierte piruvato en acetil-CoA, alfa-cetoglutarato deshidrogenasa en ciclo de Krebs, y transcetolasa en vía de pentosas fosfato que genera NADPH necesario para regeneración de glutatión reducido. Durante metabolismo de alcohol, conversión de etanol a acetaldehído y acetaldehído a acetato genera cantidades masivas de NADH que inhiben piruvato deshidrogenasa y otras deshidrogenasas NAD+-dependientes, comprometiendo metabolismo oxidativo y favoreciendo acumulación de piruvato. La provisión de tiamina en forma de benfotiamina puede favorecer actividad de enzimas tiamina-dependientes durante estrés metabólico asociado con metabolismo de alcohol, y puede modular vías metabólicas que generan productos finales de glicación avanzada mediante efectos sobre desviación de metabolitos intermediarios a vías que no generan estos compuestos reactivos.
Vitamina B6 (P5P, forma activa)
El piridoxal-5-fosfato es forma coenzimática activa de vitamina B6 que participa como cofactor de más de ciento cuarenta enzimas que catalizan reacciones de transaminación, decarboxilación, racemización y otras modificaciones de aminoácidos. Durante metabolismo de aminoácidos que es incrementado durante exposición a alcohol debido a inhibición de gluconeogénesis por NADH elevado favoreciendo catabolismo proteico, transaminasas dependientes de piridoxal-5-fosfato catalizan transferencia de grupos amino entre aminoácidos y alfa-cetoácidos, participando en interconversión de aminoácidos y generación de intermediarios que alimentan ciclo de Krebs. El piridoxal-5-fosfato es cofactor de serina hidroximetiltransferasa que cataliza conversión de serina en glicina proporcionando grupos metilo para síntesis de purinas y timidilato, y generando glicina que es precursor de glutatión junto con glutamato y cisteína. La enzima cistationina beta-sintasa que cataliza primer paso en transulfuración de homocisteína a cisteína requiere piridoxal-5-fosfato, estableciendo que disponibilidad de vitamina B6 influye en síntesis endógena de cisteína que puede ser limitante para síntesis de glutatión cuando metionina es abundante pero cisteína dietética es limitada. El piridoxal-5-fosfato también participa en síntesis de neurotransmisores incluyendo serotonina, dopamina y GABA mediante decarboxilasas de aminoácidos aromáticos que convierten 5-hidroxitriptófano en serotonina, L-DOPA en dopamina, y glutamato en GABA, modulando neurotransmisión que puede ser alterada durante exposición a alcohol.
Vitamina B12 (metilcobalamina)
La metilcobalamina es forma coenzimática de vitamina B12 que actúa como cofactor de metionina sintasa, enzima que cataliza transferencia de grupo metilo desde 5-metiltetrahidrofolato a homocisteína regenerando metionina y tetrahidrofolato. Esta reacción enlaza metabolismo de folato con metabolismo de metionina y homocisteína, siendo crítica para regeneración de tetrahidrofolato que es necesario para síntesis de purinas y timidilato requeridos para replicación de ADN, y para mantenimiento de pools de metionina que es precursor de S-adenosilmetionina que es donador universal de grupos metilo en reacciones de metilación incluyendo metilación de ADN, proteínas y lípidos. Durante metabolismo de alcohol, estrés oxidativo y alteraciones metabólicas pueden comprometer función de metionina sintasa y ciclo de metilación, y homocisteína puede acumularse cuando regeneración a metionina es insuficiente o cuando transulfuración a cisteína es limitada por disponibilidad de piridoxal-5-fosfato. La provisión de metilcobalamina puede favorecer actividad de metionina sintasa asegurando que cofactor está disponible en forma activa, aunque función de enzima también depende de estado redox apropiado de cobalamina que puede ser comprometido por estrés oxidativo severo. La adenosilcobalamina que es otra forma coenzimática de B12 actúa como cofactor de metilmalonil-CoA mutasa que participa en metabolismo de ácidos grasos de cadena impar y aminoácidos de cadena ramificada, aunque metilcobalamina no participa directamente en esta reacción, conversión entre formas de cobalamina puede ocurrir intracelularmente.
Soporte a capacidad metabólica hepática de detoxificación
La combinación sinérgica de dihidromiricetina, NACET y vitaminas del complejo B en formas optimizadas respalda capacidad del hígado de procesar etanol y metabolitos asociados mediante modulación coordinada de enzimas de fase I y fase II que catalizan oxidación y conjugación de compuestos xenobióticos. La dihidromiricetina modula actividad de alcohol deshidrogenasa y aldehído deshidrogenasa que catalizan conversión secuencial de etanol a acetaldehído y acetaldehído a acetato, mientras NACET proporciona cisteína biodisponible para síntesis de glutatión que actúa como cofactor de glutatión S-transferasas que conjugan acetaldehído y otros electrófilos facilitando eliminación. La benfotiamina proporciona tiamina pirofosfato que es cofactor de enzimas que participan en metabolismo de acetato generado durante oxidación de alcohol, incluyendo acetil-CoA sintetasa que convierte acetato en acetil-CoA que puede ser oxidado en ciclo de Krebs o utilizado en síntesis de lípidos y colesterol. El extracto de jengibre modula expresión de enzimas de fase II mediante activación de vías de señalización que inducen expresión de glutatión S-transferasas, UDP-glucuronosiltransferasas y sulfotransferasas, incrementando capacidad hepática de conjugar metabolitos reactivos con glutatión, ácido glucurónico o sulfato generando compuestos hidrosolubles excretables en orina o bilis. La provisión coordinada de cofactores vitamínicos en formas bioactivas asegura que enzimas que requieren tiamina pirofosfato, piridoxal-5-fosfato y metilcobalamina operan a capacidad óptima durante demanda metabólica incrementada asociada con procesamiento de alcohol, favoreciendo conversión eficiente de etanol a metabolitos menos reactivos y su eliminación subsecuente mediante rutas de excreción renal y biliar.
Optimización de homeostasis redox y neutralización de especies reactivas
La formulación integra precursores de glutatión, moduladores de enzimas antioxidantes endógenas y compuestos con actividad antioxidante directa estableciendo protección multiestrato contra estrés oxidativo generado durante metabolismo de alcohol. El NACET proporciona cisteína que es precursor limitante para síntesis de glutatión en hepatocitos donde consumo de glutatión es incrementado durante metabolismo de acetaldehído mediante conjugación catalizada por glutatión S-transferasas y mediante neutralización de peróxidos por glutatión peroxidasas, mientras ácido piroglutámico participa en ciclo gamma-glutamil favoreciendo regeneración de glutamato desde 5-oxoprolina que puede acumularse durante degradación acelerada de glutatión. La dihidromiricetina exhibe actividad antioxidante directa mediante neutralización de radicales libres incluyendo radicales hidroxilo y superóxido generados durante metabolismo oxidativo de etanol por sistema microsomal de oxidación de etanol que involucra citocromo P450 2E1, y mediante quelación de metales de transición que catalizan reacciones de Fenton generando especies reactivas. Los gingeroles y shogaoles del extracto de jengibre actúan como antioxidantes fenólicos neutralizando radicales lipoperoxilo que propagan peroxidación lipídica en membranas celulares, y modulan expresión de enzimas antioxidantes endógenas incluyendo superóxido dismutasas, catalasa y glutatión peroxidasas mediante activación de Nrf2 que es factor de transcripción maestro regulando respuesta adaptativa al estrés oxidativo. Las vitaminas del complejo B participan en regeneración de capacidad antioxidante mediante soporte a metabolismo energético que proporciona NADPH necesario para regeneración de glutatión reducido desde forma oxidada por glutatión reductasa, estableciendo que optimización de homeostasis redox requiere no solo neutralización de especies reactivas sino también mantenimiento de pools de reductores celulares que permiten ciclos continuos de protección antioxidante.
Modulación de inflamación hepática y sistémica
La combinación de extracto de jengibre estandarizado con dihidromiricetina y precursores de glutatión establece soporte a modulación de respuesta inflamatoria que puede ser activada durante metabolismo de alcohol mediante generación de acetaldehído que forma aductos con proteínas generando neoantígenos que activan sistema inmune, y mediante estrés oxidativo que activa vías de señalización proinflamatoria. Los gingeroles inhiben ciclooxigenasa-2 que cataliza síntesis de prostaglandinas proinflamatorias incluyendo PGE2 que media vasodilatación, incremento en permeabilidad vascular y sensibilización de nociceptores, y 5-lipooxigenasa que cataliza síntesis de leucotrienos que son quimioatractantes potentes reclutando neutrófilos y otros leucocitos a sitios de inflamación. La inhibición de NF-kappaB por compuestos del jengibre y dihidromiricetina reduce translocación nuclear de este factor de transcripción que regula expresión de genes que codifican citoquinas proinflamatorias incluyendo TNF-alfa, IL-1beta e IL-6 que activan células de Kupffer que son macrófagos residentes en hígado, y células estrelladas hepáticas que pueden ser activadas a fenotipo fibrogénico produciendo colágeno excesivo. El glutatión generado desde precursores proporcionados por NACET modula señalización redox-sensible incluyendo activación de NF-kappaB y AP-1 que son factores de transcripción que responden a cambios en estado redox celular, estableciendo que mantenimiento de homeostasis redox mediante provisión de glutatión tiene efectos secundarios sobre modulación de inflamación más allá de neutralización directa de especies reactivas. La modulación coordinada de múltiples puntos en cascada inflamatoria mediante inhibición de síntesis de mediadores lipídicos, reducción de expresión de citoquinas y modulación de estado redox que controla activación de vías de señalización establece aproximación integral a soporte de homeostasis inflamatoria durante exposición a alcohol.
Soporte a función mitocondrial y metabolismo energético
La provisión de cofactores vitamínicos del complejo B en formas bioactivas que no requieren conversión enzimática favorece función de enzimas mitocondriales que catalizan pasos críticos en metabolismo oxidativo de carbohidratos, lípidos y aminoácidos que genera ATP mediante fosforilación oxidativa. La benfotiamina proporciona tiamina pirofosfato que es cofactor de piruvato deshidrogenasa que cataliza descarboxilación oxidativa de piruvato generando acetil-CoA que alimenta ciclo de Krebs, alfa-cetoglutarato deshidrogenasa que cataliza paso limitante en ciclo de Krebs generando succinil-CoA y NADH, y complejo de deshidrogenasa de alfa-cetoácidos de cadena ramificada que procesa leucina, isoleucina y valina. El piridoxal-5-fosfato participa en transaminación de aminoácidos generando alfa-cetoácidos que pueden alimentar ciclo de Krebs como intermediarios anaplerósicos, mientras metilcobalamina participa en metabolismo de propionil-CoA derivado de oxidación de ácidos grasos de cadena impar y aminoácidos mediante conversión de metilmalonil-CoA a succinil-CoA que entra en ciclo de Krebs. Durante metabolismo de alcohol, generación masiva de NADH desde oxidación de etanol a acetaldehído y acetaldehído a acetato incrementa ratio NADH/NAD+ que inhibe deshidrogenasas NAD+-dependientes en ciclo de Krebs comprometiendo generación de ATP y favoreciendo desviación de piruvato a lactato más que oxidación a acetil-CoA, fenómeno que puede comprometer metabolismo energético particularmente en tejidos con alta demanda como cerebro y corazón. La provisión de cofactores que mantienen actividad de enzimas mitocondriales durante perturbación metabólica asociada con alcohol, combinada con protección antioxidante que previene daño a complejos respiratorios por especies reactivas, favorece mantenimiento de capacidad de generación de ATP que es crítica para función celular óptima en todos los tejidos.
Favorecimiento de procesamiento de amonio en ciclo de urea
La provisión de L-ornitina como sustrato para ornitina transcarbamilase que cataliza primer paso comprometido de ciclo de urea respalda capacidad hepática de convertir amonio tóxico en urea que es compuesto hidrosoluble no tóxico excretable por riñón, función particularmente relevante durante metabolismo de alcohol donde generación de acetaldehído y acumulación de NADH inhiben gluconeogénesis y favorecen catabolismo de aminoácidos incrementando liberación de grupos amino que son convertidos a amonio mediante desaminación. El ciclo de urea opera en hepatocitos donde ornitina transcarbamilase mitocondrial condensa ornitina con carbamil fosfato formando citrulina, citrulina es exportada a citoplasma donde argininosuccinato sintetasa condensa citrulina con aspartato formando argininosuccinato, argininosuccinasa escinde argininosuccinato generando arginina y fumarato, y arginasa hidroliza arginina regenerando ornitina y liberando urea que es excretada. La disponibilidad de ornitina puede ser limitante para velocidad de ciclo particularmente cuando generación de amonio es incrementada y cuando síntesis endógena de ornitina desde glutamato mediante vía de ornitina sintasa es insuficiente para demanda. Las vitaminas del complejo B participan en metabolismo de aminoácidos que alimenta ciclo de urea mediante transaminación que transfiere grupos amino a glutamato formando alfa-cetoácidos que pueden ser oxidados o convertidos en glucosa, y glutamato entonces transfiere grupo amino a oxaloacetato formando aspartato que es sustrato directo de argininosuccinato sintetasa. La integración de provisión de ornitina con cofactores que optimizan transaminación y metabolismo de aminoácidos establece soporte coordinado a procesamiento de amonio que puede prevenir acumulación que compromete función del sistema nervioso central donde amonio interfiere con neurotransmisión y metabolismo energético cerebral.
Modulación de función gastrointestinal y motilidad
El extracto de jengibre con gingeroles y shogaoles modula función del tracto gastrointestinal mediante efectos sobre receptores serotoninérgicos particularmente 5-HT3 que median náusea y vómito cuando activados en área postrema del tronco cerebral, y receptores colinérgicos que modulan contracción de músculo liso intestinal determinando peristalsis y velocidad de tránsito. Durante exposición a alcohol, irritación de mucosa gástrica por etanol que es solvente orgánico que disuelve lípidos de membranas celulares, retraso en vaciamiento gástrico, y acumulación de acetaldehído que tiene efectos eméticos directos pueden comprometer función digestiva y generar manifestaciones gastrointestinales incluyendo náusea, distensión y malestar epigástrico. Los compuestos del jengibre favorecen vaciamiento gástrico mediante estimulación de contracciones antrales coordinadas que propulsan contenido gástrico hacia duodeno, y modulan tono del esfínter pilórico que regula flujo desde estómago a intestino delgado. La actividad antioxidante y antiinflamatoria de gingeroles también protege mucosa gástrica de daño oxidativo e inflamación inducidos por alcohol mediante neutralización de especies reactivas generadas en células epiteliales y mediante inhibición de producción de citoquinas proinflamatorias que pueden alterar integridad de barrera mucosa. La modulación de secreción de ácido gástrico y pepsina por compuestos del jengibre puede influir en digestión de proteínas y en ambiente de pH gástrico que determina actividad de enzimas digestivas, estableciendo efectos sobre múltiples aspectos de función gastrointestinal que pueden ser comprometidos durante exposición a alcohol.
Soporte a homeostasis de neurotransmisores y función neurológica
La provisión de piridoxal-5-fosfato y metilcobalamina que participan en síntesis y metabolismo de neurotransmisores favorece mantenimiento de función neurológica durante exposición a alcohol que modula múltiples sistemas de neurotransmisión mediante efectos sobre receptores GABA, glutamato, serotonina y dopamina. El piridoxal-5-fosfato es cofactor de decarboxilasa de ácido glutámico que convierte glutamato en GABA que es neurotransmisor inhibitorio principal en sistema nervioso central modulando excitabilidad neuronal, de decarboxilasa de aminoácidos aromáticos que convierte L-DOPA en dopamina y 5-hidroxitriptófano en serotonina, y de serina hidroximetiltransferasa que genera glicina que actúa como neurotransmisor inhibitorio en médula espinal y tronco cerebral. La metilcobalamina participa en metabolismo de homocisteína mediante metionina sintasa que regenera metionina, precursor de S-adenosilmetionina que es donador de grupos metilo en reacciones de metilación incluyendo síntesis de fosfatidilcolina que es componente mayoritario de membranas neuronales y mielina, y metilación de neurotransmisores que modula su actividad y degradación. La dihidromiricetina modula receptores GABA-A mediante mecanismo que contrarresta efectos de etanol sobre estos receptores que normalmente potencia transmisión GABAérgica generando efectos sedantes y ansiolíticos, estableciendo que DHM puede modular algunos aspectos de efectos de alcohol sobre sistema nervioso central aunque mecanismos precisos requieren caracterización adicional. El mantenimiento de síntesis apropiada de neurotransmisores mediante provisión de cofactores vitamínicos, combinado con protección antioxidante de neuronas mediante glutatión que neutraliza especies reactivas que pueden dañar membranas neuronales ricas en lípidos insaturados susceptibles a peroxidación, establece soporte integral a función neurológica durante perturbación metabólica asociada con alcohol.
Protección de integridad de membranas celulares y función de barrera
La combinación de antioxidantes que neutralizan radicales lipoperoxilo con precursores de glutatión y cofactores que participan en síntesis de fosfolípidos favorece mantenimiento de integridad estructural de membranas celulares que pueden ser comprometidas durante metabolismo de alcohol mediante peroxidación lipídica iniciada por especies reactivas de oxígeno. Las membranas biológicas están compuestas predominantemente de fosfolípidos que contienen ácidos grasos insaturados particularmente en posición sn-2 de glicerol, y estos dobles enlaces carbono-carbono son susceptibles a ataque por radicales libres iniciando reacción en cadena de peroxidación lipídica donde radicales lipoperoxilo generados propagan daño a lípidos adyacentes generando aldehídos reactivos incluyendo malondialdehído y 4-hidroxinonenal que forman aductos con proteínas de membrana comprometiendo función. Los gingeroles y shogaoles actúan como antioxidantes fenólicos que donan hidrógeno a radicales lipoperoxilo terminando reacción en cadena, mientras glutatión generado desde NACET actúa como cofactor de glutatión peroxidasas que reducen hidroperóxidos lipídicos a alcoholes menos reactivos antes de que propaguen peroxidación. La metilcobalamina participa en regeneración de metionina que es precursor de S-adenosilmetionina que dona grupos metilo en reacción catalizada por fosfatidiletanolamina N-metiltransferasa que convierte fosfatidiletanolamina en fosfatidilcolina, estableciendo que homeostasis de metilación influye en composición de fosfolípidos de membrana. La protección de integridad de membranas es particularmente relevante en hepatocitos donde metabolismo intenso de alcohol genera estrés oxidativo elevado, y en membranas mitocondriales donde peroxidación puede comprometer función de complejos respiratorios embebidos en membrana interna mitocondrial, estableciendo que mantenimiento de integridad de membranas es crítico para preservación de función celular durante exposición a alcohol.
¿Sabías que el hígado humano puede procesar aproximadamente siete a diez gramos de etanol puro por hora, equivalente a menos de una bebida estándar, estableciendo un límite metabólico fijo que no puede acelerarse significativamente?
La velocidad de metabolismo de alcohol está determinada principalmente por cantidad de alcohol deshidrogenasa presente en hepatocitos, y esta cantidad es relativamente constante en individuos no adaptados. Aunque consumo crónico de alcohol puede inducir expresión de citocromo P450 2E1 que proporciona vía metabólica alternativa incrementando ligeramente capacidad total, la vía principal a través de alcohol deshidrogenasa opera cerca de su capacidad máxima incluso con concentraciones moderadas de etanol. Esto significa que consumir múltiples bebidas rápidamente genera acumulación de etanol en sangre dado que ingesta excede dramáticamente capacidad de metabolismo, y que spacing de consumo a través de varias horas permite que metabolismo procese alcohol conforme es consumido manteniendo concentraciones sanguíneas más bajas. La provisión de cofactores como vitaminas del complejo B no incrementa velocidad máxima de alcohol deshidrogenasa pero asegura que enzimas operan óptimamente dentro de sus limitaciones cinéticas inherentes, y que pasos subsecuentes en metabolismo de acetaldehído no son limitados por disponibilidad de cofactores.
¿Sabías que el acetaldehído generado durante metabolismo de alcohol es hasta treinta veces más reactivo que el etanol mismo, formando aductos con proteínas y ADN que contribuyen a efectos adversos?
El acetaldehído contiene grupo aldehído altamente electrofílico que reacciona con grupos nucleofílicos en proteínas incluyendo grupos amino de lisina y grupos tiol de cisteína, formando enlaces covalentes que modifican estructura y función de proteínas. Estos aductos acetaldehído-proteína pueden ser reconocidos como neoantígenos por sistema inmune generando respuesta inflamatoria, y pueden comprometer función de enzimas críticas cuando residuos en sitio activo son modificados. El acetaldehído también forma aductos con bases de ADN particularmente guanina, generando lesiones que requieren reparación mediante sistemas de reparación de ADN y que si no son reparadas apropiadamente pueden contribuir a mutagénesis. La aldehído deshidrogenasa que convierte acetaldehído a acetato es crítica para prevenir acumulación de este metabolito altamente reactivo, y polimorfismos genéticos que reducen actividad de esta enzima generan acumulación de acetaldehído incluso con consumo moderado de alcohol. La provisión de precursores de glutatión como NACET favorece conjugación de acetaldehído mediante glutatión S-transferasas que catalizan adición nucleofílica de glutatión a grupo aldehído, proporcionando vía de eliminación adicional que complementa oxidación por aldehído deshidrogenasa.
¿Sabías que el NACET como éster lipofílico de N-acetilcisteína puede atravesar membranas celulares hasta cien veces más eficientemente que N-acetilcisteína estándar debido a neutralización de carga del grupo carboxilo?
La N-acetilcisteína en pH fisiológico existe predominantemente como anión debido a ionización de grupo carboxilo, y esta carga negativa impide permeabilidad a través de bicapa lipídica de membranas celulares que es ambiente hidrofóbico que excluye moléculas cargadas. El NACET mediante esterificación de grupo carboxilo con etanol neutraliza esta carga generando molécula que puede particionar en ambiente lipídico de membranas y atravesarlas mediante difusión pasiva sin requerir transportadores. Una vez dentro de células, esterasas citosólicas hidrolizan éster liberando N-acetilcisteína en compartimento intracelular donde puede ser deacetilada liberando cisteína para síntesis de glutatión, o puede ser exportada a compartimentos específicos como mitocondrias. Esta ventaja en biodisponibilidad celular es particularmente relevante para células con expresión limitada de transportadores de cisteína o N-acetilcisteína, y para provisión de precursores de glutatión a mitocondrias donde síntesis de glutatión ocurre localmente y donde glutatión mitocondrial es crítico para protección de cadena respiratoria de estrés oxidativo generado durante fosforilación oxidativa que es incrementado durante metabolismo de alcohol.
¿Sabías que durante metabolismo de una sola bebida alcohólica el hígado puede consumir más de la mitad de sus reservas totales de glutatión en conjugación de acetaldehído y neutralización de especies reactivas?
El glutatión hepático existe en concentraciones de cinco a diez milimolar en hepatocitos, representando reservorio sustancial de capacidad antioxidante y de conjugación. Sin embargo, durante metabolismo de alcohol la generación de acetaldehído que es conjugado por glutatión S-transferasas, producción de peróxidos por sistema microsomal de oxidación de etanol que involucra citocromo P450 2E1, y generación de radicales durante oxidación de acetaldehído por aldehído deshidrogenasa consumen glutatión rápidamente. La síntesis de novo de glutatión mediante glutamato-cisteína ligasa y glutatión sintetasa requiere varias horas para repleción completa de pools depletados, haciendo que exposición repetida a alcohol en intervalos cortos puede generar depleción acumulativa que compromete capacidad de protección en exposiciones subsecuentes. La provisión de precursores de glutatión mediante NACET que proporciona cisteína y ácido piroglutámico que participa en ciclo gamma-glutamil favorece síntesis acelerada de glutatión durante y después de metabolismo de alcohol, aunque velocidad de síntesis aún está limitada por capacidad catalítica de enzimas de síntesis que no pueden ser incrementadas agudamente. Esta dependencia crítica en glutatión para procesamiento de alcohol explica por qué depleción de glutatión por exposición previa a otros xenobióticos, malnutrición que limita disponibilidad de precursores, o polimorfismos que reducen expresión de enzimas de síntesis de glutatión incrementan vulnerabilidad a efectos adversos de alcohol.
¿Sabías que la dihidromiricetina puede modular receptores GABA-A mediante mecanismo que contrarresta algunos efectos de etanol sobre estos receptores sin generar efectos sedantes independientes?
El etanol potencia transmisión GABAérgica mediante unión a sitio específico en receptores GABA-A que incrementa probabilidad de apertura de canal y duración de aperturas cuando GABA se une, generando entrada incrementada de cloruro que hiperpolariza neuronas reduciendo excitabilidad. La dihidromiricetina se une a sitio diferente en receptor GABA-A y modula efectos de etanol sobre receptor mediante mecanismo que no está completamente caracterizado pero que puede involucrar cambios conformacionales que reducen capacidad de etanol de potenciar transmisión GABAérgica. Estudios preclínicos sugieren que DHM reduce algunos efectos conductuales de etanol incluyendo ataxia y sedación en modelos animales cuando administrada antes o después de exposición a alcohol, aunque traducción de estos efectos a humanos requiere caracterización adicional. Crítico es que DHM no activa receptores GABA-A independientemente como hacen benzodiacepinas o barbitúricos, sino que modula efectos de etanol cuando ambos están presentes, estableciendo perfil de seguridad potencialmente superior dado que no genera efectos depresores del sistema nervioso central cuando alcohol no está presente. Este mecanismo es distinto de modulación de metabolismo de alcohol por DHM y representa efecto adicional que puede contribuir a experiencia subjetiva modificada durante y después de consumo de alcohol.
¿Sabías que el metabolismo de alcohol genera ratio NADH/NAD+ incrementado que puede alcanzar diez veces el valor normal en hepatocitos, alterando fundamentalmente múltiples vías metabólicas simultáneamente?
La oxidación de etanol a acetaldehído por alcohol deshidrogenasa y acetaldehído a acetato por aldehído deshidrogenasa ambas generan NADH desde NAD+, y cuando metabolismo de alcohol es intenso la producción de NADH excede capacidad de cadena respiratoria mitocondrial de oxidar NADH de vuelta a NAD+. Este incremento dramático en ratio NADH/NAD+ inhibe todas las deshidrogenasas NAD+-dependientes que catalizan reacciones oxidativas, incluyendo lactato deshidrogenasa que convierte lactato a piruvato resultando en acumulación de lactato, malato deshidrogenasa en ciclo de Krebs que convierte malato a oxaloacetato generando acumulación de malato, y glicerol-3-fosfato deshidrogenasa que participa en lanzadera de equivalentes reductores entre citoplasma y mitocondrias. La inhibición de gluconeogénesis por NADH elevado que inhibe conversión de lactato a piruvato y de malato a oxaloacetato favorece hipoglucemia particularmente en individuos que han ayunado, mientras que inhibición de beta-oxidación de ácidos grasos por NADH elevado que inhibe 3-hidroxiacil-CoA deshidrogenasa favorece acumulación de lípidos en hepatocitos. La provisión de benfotiamina que proporciona tiamina pirofosfato favorece desviación de piruvato hacia descarboxilación oxidativa por piruvato deshidrogenasa más que reducción a lactato, aunque esta enzima también es inhibida por NADH elevado estableciendo limitación. La regeneración de NAD+ mediante oxidación de NADH en cadena respiratoria mitocondrial es crítica para restauración de homeostasis metabólica, y protección de función mitocondrial mediante antioxidantes que previenen daño a complejos respiratorios favorece capacidad de oxidación de NADH.
¿Sabías que los gingeroles del jengibre pueden inhibir ciclooxigenasa-2 con potencia similar a algunos compuestos farmacológicos pero con perfil de selectividad diferente que minimiza efectos sobre mucosa gástrica?
La ciclooxigenasa-2 es isoforma inducible de ciclooxigenasa que es expresada en respuesta a estímulos inflamatorios incluyendo citoquinas y estrés oxidativo, catalizando conversión de ácido araquidónico a prostaglandinas incluyendo PGE2 que media vasodilatación, dolor e inflamación. Los gingeroles inhiben actividad catalítica de COX-2 mediante mecanismos que incluyen reducción de expresión de enzima mediante efectos sobre NF-kappaB que regula transcripción de gen que codifica COX-2, y posiblemente mediante efectos sobre actividad de enzima aunque mecanismos moleculares precisos están siendo caracterizados. A diferencia de inhibidores selectivos de COX-2 sintéticos que pueden incrementar riesgo cardiovascular mediante inhibición de prostaciclina que es vasodilatador y antiagregante plaquetario producido por endotelio vascular, los gingeroles exhiben múltiples efectos sobre vías relacionadas incluyendo inhibición de lipooxigenasas y modulación de producción de tromboxano que pueden balancear efectos sobre homeostasis cardiovascular. Los gingeroles también no comprometen significativamente síntesis de prostaglandinas que protegen mucosa gástrica dado que estas son producidas constitutivamente por COX-1 más que COX-2 inducible, estableciendo perfil de seguridad gastrointestinal potencialmente superior comparado con inhibidores no selectivos de ciclooxigenasa. Durante metabolismo de alcohol donde inflamación hepática puede ser activada por acetaldehído y especies reactivas, modulación de COX-2 por gingeroles puede favorecer reducción de producción de mediadores proinflamatorios sin comprometer funciones fisiológicas de prostaglandinas generadas constitutivamente.
¿Sabías que la benfotiamina puede alcanzar concentraciones intracelulares de tiamina hasta cinco veces más elevadas que tiamina hidrocloruro debido a su lipofilicidad que favorece absorción y retención celular?
La tiamina hidrocloruro que es forma estándar de suplementación de vitamina B1 es molécula altamente polar que requiere transportadores específicos para absorción intestinal y entrada a células, y estos transportadores tienen capacidad limitada estableciendo saturabilidad donde incrementos en dosis más allá de cierto punto no incrementan proporcionalmente absorción. La benfotiamina mediante sustitución de grupo hidroxilo con grupo S-acil incrementa lipofilicidad permitiendo absorción por difusión pasiva a través de membranas intestinales sin dependencia completa en transportadores, y permeabilidad celular incrementada que favorece entrada a tejidos. Una vez absorbida, benfotiamina es convertida a tiamina mediante hidrólisis de éster, y tiamina es entonces fosforilada formando tiamina pirofosfato que es forma coenzimática activa. La acumulación intracelular incrementada de tiamina desde benfotiamina resulta en disponibilidad mayor de tiamina pirofosfato para enzimas que la requieren como cofactor, potencialmente saturando sitios de unión y asegurando que actividad de enzimas no es limitada por disponibilidad de cofactor. Durante metabolismo de alcohol donde demanda de tiamina pirofosfato es incrementada dado que enzimas tiamina-dependientes incluyendo transcetolasa participan en metabolismo de intermediarios generados durante perturbación metabólica por NADH elevado, la provisión de tiamina en forma que genera niveles intracelulares elevados favorece mantenimiento de actividad enzimática apropiada. La benfotiamina también puede tener efectos adicionales más allá de provisión de tiamina incluyendo activación de transcetolasa que desvía intermediarios glucolíticos a vía de pentosas fosfato que genera NADPH necesario para regeneración de glutatión reducido.
¿Sabías que el ácido piroglutámico se acumula cuando síntesis de glutatión es inhibida o cuando degradación de glutatión es acelerada, sirviendo como indicador metabólico de turnover de glutatión?
El ácido piroglutámico es generado durante ciclo gamma-glutamil cuando gamma-glutamiltranspeptidasa en membrana celular escinde glutamato N-terminal de glutatión durante degradación extracelular, y glutamato cíclico resultante es convertido a ácido piroglutámico mediante ciclización espontánea. El ácido piroglutámico debe ser convertido de vuelta a glutamato mediante 5-oxoprolinasa que utiliza ATP para abrir anillo y regenerar forma de cadena abierta, completando ciclo que permite reutilización de glutamato en síntesis de nuevo glutatión. Cuando demanda de glutatión es incrementada dramáticamente como durante metabolismo de alcohol donde conjugación de acetaldehído y neutralización de especies reactivas consumen glutatión rápidamente, degradación acelerada de glutatión genera ácido piroglutámico más rápido que 5-oxoprolinasa puede procesarlo, resultando en acumulación. Alternativamente, cuando síntesis de glutatión es inhibida por deficiencia de precursores o por inhibición de gamma-glutamil-cisteína ligasa, el ácido piroglutámico generado durante degradación normal de glutatión no es reutilizado eficientemente porque síntesis de nuevo glutatión es comprometida. La provisión de ácido piroglutámico exógeno puede proporcionar sustrato adicional para 5-oxoprolinasa facilitando regeneración de glutamato que puede entonces ser utilizado en síntesis de glutatión, aunque efectividad depende de disponibilidad de cisteína y glicina que son otros precursores necesarios y de capacidad catalítica de enzimas de síntesis de glutatión.
¿Sabías que la ornitina participa en ciclo de urea que consume cuatro equivalentes de ATP de alta energía para convertir una molécula de amonio en urea, haciendo que procesamiento de amonio es metabólicamente costoso?
El ciclo de urea es vía metabólica que opera principalmente en hígado convirtiendo amonio tóxico generado durante catabolismo de aminoácidos en urea que es compuesto no tóxico que puede ser excretado por riñón. El ciclo requiere condensación de carbamil fosfato con ornitina formando citrulina en paso catalizado por ornitina transcarbamilase, condensación de citrulina con aspartato formando argininosuccinato consumiendo ATP en paso catalizado por argininosuccinato sintetasa, escisión de argininosuccinato a arginina y fumarato, e hidrólisis de arginina a urea y ornitina regenerando ornitina para inicio de nuevo ciclo. La síntesis de carbamil fosfato desde bicarbonato y amonio consume dos ATP, mientras condensación de citrulina con aspartato consume un ATP adicional que es escindido a AMP y pirofosfato equivalente a dos equivalentes de ATP, estableciendo costo total de cuatro ATP de alta energía por molécula de urea producida. Este costo energético sustancial ilustra importancia de conversión de amonio que es altamente tóxico particularmente para sistema nervioso donde interfiere con neurotransmisión glutamatérgica y metabolismo energético, en compuesto que puede ser eliminado seguramente. Durante metabolismo de alcohol donde catabolismo de aminoácidos es incrementado debido a inhibición de gluconeogénesis por NADH elevado que favorece utilización de aminoácidos para generación de energía, producción de amonio es incrementada y ciclo de urea opera a capacidad elevada. La provisión de ornitina puede favorecer capacidad de ciclo particularmente cuando generación de amonio excede síntesis endógena de ornitina desde glutamato, aunque efectividad también depende de disponibilidad de carbamil fosfato y aspartato que son otros sustratos del ciclo.
¿Sabías que el piridoxal-5-fosfato participa en más de ciento cuarenta reacciones enzimáticas diferentes, más que cualquier otro cofactor vitamínico, debido a versatilidad química del grupo aldehído de piridoxal?
El piridoxal-5-fosfato contiene grupo aldehído reactivo que forma base de Schiff mediante condensación con grupos amino de aminoácidos en sitios activos de enzimas, generando intermediario que es estabilizado por resonancia con sistema de anillo piridina y que puede ser manipulado mediante catálisis enzimática para promover múltiples tipos de transformaciones químicas. Las transaminasas utilizan PLP para transferir grupos amino entre aminoácidos y alfa-cetoácidos mediante formación de intermediario piridoxamina fosfato, decarboxilasas utilizan PLP para estabilizar carbanión generado durante remoción de grupo carboxilo permitiendo liberación de CO2, y enzimas de eliminación utilizan PLP para promover escisión de enlaces carbono-carbono adyacentes a grupo amino. Esta versatilidad química permite que PLP participe en metabolismo de todos los aminoácidos incluyendo síntesis, degradación e interconversión, y en síntesis de neurotransmisores incluyendo serotonina, dopamina, norepinefrina, GABA e histamina mediante decarboxilación de precursores aminoácidos. Durante metabolismo de alcohol donde metabolismo de aminoácidos es perturbado por NADH elevado que inhibe gluconeogénesis favoreciendo catabolismo de aminoácidos, y donde síntesis de neurotransmisores puede ser comprometida, provisión de piridoxal-5-fosfato en forma bioactiva que no requiere fosforilación adicional asegura que enzimas dependientes de PLP operan apropiadamente. La forma P5P es superior a piridoxina que requiere fosforilación por piridoxal quinasa que puede ser limitante, y es particularmente relevante en individuos con polimorfismos que reducen actividad de esta enzima comprometiendo conversión de piridoxina a forma activa.
¿Sabías que la metilcobalamina participa en metionina sintasa que es única enzima en mamíferos que requiere vitamina B12 como cofactor junto con adenosilcobalamina en metilmalonil-CoA mutasa?
A diferencia de otras vitaminas del complejo B que participan como cofactores en múltiples enzimas, vitamina B12 participa únicamente en dos reacciones en mamíferos, ilustrando especificidad extrema de requerimiento. La metionina sintasa cataliza transferencia de grupo metilo desde 5-metiltetrahidrofolato a homocisteína regenerando metionina y tetrahidrofolato, reacción que es crítica para enlazar metabolismo de folato con metabolismo de metionina y para regeneración de tetrahidrofolato que es necesario para síntesis de purinas y timidilato requeridos para replicación de ADN. La metilcobalamina en sitio activo de metionina sintasa alterna entre estados metil-cobalamina y cob(I)alamina durante catálisis, y cob(I)alamina es altamente susceptible a oxidación a cob(II)alamina que es forma inactiva. La reactivación de metionina sintasa cuando cobalamina es oxidada requiere S-adenosilmetionina como donador de grupo metilo en reacción catalizada por dominio de reactivación de propia metionina sintasa, estableciendo ciclo donde metionina es tanto producto como cofactor necesario para mantenimiento de actividad enzimática. Durante estrés oxidativo asociado con metabolismo de alcohol, oxidación de cobalamina puede ser incrementada comprometiendo actividad de metionina sintasa y resultando en acumulación de homocisteína y depleción de 5-metiltetrahidrofolato en forma conocida como trampa de metilo donde folato queda atrapado en forma metilada que no puede ser utilizada en otras reacciones de folato. La provisión de metilcobalamina puede favorecer mantenimiento de actividad de metionina sintasa aunque función también depende de protección contra oxidación de cofactor que requiere homeostasis redox apropiada.
¿Sabías que el extracto de jengibre puede modular vaciamiento gástrico mediante efectos sobre receptores 5-HT3 y muscarínicos que regulan motilidad del antro gástrico y tono del esfínter pilórico?
El vaciamiento gástrico es proceso coordinado donde contenido gástrico es propulsado desde antro a través de esfínter pilórico hacia duodeno mediante contracciones peristálticas que son reguladas por sistemas nerviosos intrínseco y extrínseco, y por hormonas gastrointestinales. Los gingeroles modulan receptores serotoninérgicos 5-HT3 que median efectos eméticos de serotonina liberada por células enterocromafines en mucosa gastrointestinal, actuando como antagonistas que reducen activación de nervios aferentes vagales que transmiten señales al centro del vómito en área postrema del tronco cerebral. Los compuestos del jengibre también modulan receptores muscarínicos M3 que median contracción de músculo liso gastrointestinal en respuesta a acetilcolina liberada por neuronas del plexo mientérico, favoreciendo coordinación de contracciones que propulsan contenido sin generar contracciones desorganizadas que comprometen vaciamiento. Durante consumo de alcohol, vaciamiento gástrico puede ser retrasado por efectos directos de etanol sobre motilidad gástrica y por efectos sobre sistema nervioso central que modula regulación de función gastrointestinal mediante nervio vago. El retraso en vaciamiento gástrico prolonga exposición de mucosa gástrica a alcohol que es irritante directo disolviendo lípidos de membranas celulares, y puede contribuir a náusea mediante distensión gástrica que activa mecanorreceptores. La modulación de vaciamiento gástrico por extracto de jengibre puede favorecer propulsión coordinada de contenido gástrico reduciendo distensión y exposición prolongada de mucosa a irritantes, aunque efectos deben ser balanceados dado que vaciamiento muy rápido puede generar entrada abrupta de contenido ácido a duodeno que puede generar manifestaciones.
¿Sabías que durante metabolismo intenso de alcohol el hígado puede desviar hasta ochenta por ciento de su consumo de oxígeno a sistema microsomal de oxidación de etanol que involucra citocromo P450 2E1?
El hígado en estado basal consume aproximadamente veinte por ciento del oxígeno corporal total a pesar de representar solo dos a tres por ciento de masa corporal, reflejando alta tasa metabólica. Durante metabolismo de alcohol, oxidación de etanol a acetaldehído ocurre principalmente mediante alcohol deshidrogenasa citosólica, pero cuando concentraciones de etanol son elevadas sistema microsomal de oxidación de etanol que involucra citocromo P450 2E1 en retículo endoplásmico contribuye sustancialmente. El CYP2E1 cataliza oxidación de etanol utilizando NADPH y oxígeno molecular, generando acetaldehído y agua, pero proceso es relativamente ineficiente con producción significativa de especies reactivas de oxígeno incluyendo anión superóxido y peróxido de hidrógeno como subproductos. La inducción de expresión de CYP2E1 durante consumo crónico de alcohol incrementa capacidad metabólica pero también incrementa generación de especies reactivas que pueden exceder capacidad de sistemas antioxidantes endógenos de neutralizar, contribuyendo a estrés oxidativo hepático. La desviación de consumo de oxígeno a metabolismo de alcohol puede comprometer disponibilidad de oxígeno para otras funciones mitocondriales incluyendo fosforilación oxidativa que genera ATP, y puede generar gradientes de oxígeno en lobulillo hepático donde zona perivenosa que normalmente opera con tensión de oxígeno más baja puede experimentar hipoxia relativa. La protección de función mitocondrial mediante antioxidantes que neutralizan especies reactivas generadas por CYP2E1 y que previenen daño a complejos respiratorios favorece mantenimiento de capacidad de generación de ATP durante metabolismo intenso de alcohol.
¿Sabías que la L-ornitina puede ser convertida en poliaminas incluyendo putrescina, espermidina y espermina que participan en proliferación celular y reparación tisular mediante estabilización de ADN y ARN?
La ornitina es sustrato de ornitina descarboxilasa que cataliza remoción de grupo carboxilo generando putrescina, primera poliamina en vía de síntesis que es entonces modificada mediante adición de grupos aminopropilo derivados de S-adenosilmetionina descarboxilada formando espermidina y espermina. Las poliaminas son cationes orgánicos que se unen a grupos fosfato cargados negativamente en ADN, ARN y proteínas, neutralizando cargas y estabilizando estructuras macromoleculares. Durante replicación de ADN, poliaminas estabilizan conformación de doble hélice facilitando procesividad de polimerasas, durante transcripción estabilizan complejos ARN polimerasa-ADN, y durante traducción estabilizan estructura de ribosomas y ARN de transferencia facilitando síntesis proteica. La síntesis de poliaminas es altamente regulada con expresión de ornitina descarboxilasa siendo incrementada durante proliferación celular, regeneración tisular y respuesta a estrés. Durante recuperación de exposición a alcohol donde hepatocitos pueden experimentar estrés que compromete integridad celular, síntesis de poliaminas puede respaldar reparación de membranas, regeneración de organelos y síntesis de proteínas necesarias para restauración de función. Sin embargo, síntesis de poliaminas consume S-adenosilmetionina que es también donador de grupos metilo en múltiples reacciones de metilación, estableciendo competencia entre utilización de SAM para síntesis de poliaminas versus reacciones de metilación. La provisión de metilcobalamina que participa en regeneración de metionina que es precursor de SAM puede favorecer mantenimiento de pools de SAM suficientes para ambas funciones durante periodos de demanda incrementada.
¿Sabías que los shogaoles del jengibre son formados por deshidratación de gingeroles durante procesamiento térmico o almacenamiento prolongado, y exhiben potencia incrementada en algunos ensayos de actividad biológica?
Los gingeroles contienen grupo hidroxilo y grupo cetona en posiciones específicas que bajo condiciones de calor o pH ácido pueden sufrir deshidratación mediante eliminación de agua, generando doble enlace adicional y formando shogaoles. Esta transformación química incrementa conjugación en molécula y modifica propiedades fisicoquímicas incluyendo lipofilicidad y reactividad. Los shogaoles exhiben actividad antiinflamatoria incrementada en algunos modelos mediante inhibición más potente de producción de prostaglandinas y leucotrienos comparado con gingeroles, y actividad antioxidante que puede ser superior debido a estructura electrónica modificada que facilita donación de hidrógeno a radicales libres. Los extractos de jengibre que son procesados térmicamente o que provienen de jengibre seco contienen proporción más elevada de shogaoles comparado con jengibre fresco que contiene predominantemente gingeroles, haciendo que composición de extracto influye en perfil de actividad biológica. Durante metabolismo de alcohol donde modulación de inflamación y neutralización de especies reactivas son relevantes, presencia de ambos gingeroles y shogaoles en extracto estandarizado proporciona espectro de compuestos bioactivos que pueden actuar sinérgicamente mediante múltiples mecanismos. La biodisponibilidad de shogaoles puede ser diferente comparado con gingeroles debido a diferencias en lipofilicidad y metabolismo de primer paso, aunque estudios farmacocinéticos detallados en humanos son limitados estableciendo que caracterización adicional de absorción, distribución y metabolismo es necesaria para comprensión completa de contribución relativa de diferentes compuestos en extracto.
¿Sabías que el glutatión existe en forma reducida con grupo tiol libre y forma oxidada como dímero unido por puente disulfuro, y que ratio entre formas refleja estado redox celular que modula señalización?
El glutatión reducido contiene grupo tiol de cisteína que puede ser oxidado formando puente disulfuro con otra molécula de glutatión generando glutatión disulfuro, reacción que ocurre durante neutralización de especies reactivas cuando glutatión dona electrones. El ratio glutatión reducido/glutatión oxidado en células saludables es típicamente mayor que cien a uno, estableciendo ambiente reductor que mantiene grupos tiol de proteínas en estado reducido funcional y que favorece reacciones que requieren ambiente reductor. Cambios en este ratio hacia estado más oxidado modulan función de proteínas que contienen cisteínas sensibles a redox incluyendo factores de transcripción cuya actividad de unión a ADN depende de estado redox de cisteínas en dominio de unión, quinasas y fosfatasas cuya actividad catalítica es modulada por oxidación de cisteínas en sitio activo, y canales iónicos cuya probabilidad de apertura es influida por estado redox. Durante estrés oxidativo asociado con metabolismo de alcohol, consumo de glutatión reducido en neutralización de especies reactivas y conjugación de acetaldehído genera acumulación de glutatión oxidado que si no es regenerado eficientemente por glutatión reductasa que utiliza NADPH altera ratio estableciendo estado oxidativo que puede activar vías de señalización de estrés. La provisión de precursores de glutatión mediante NACET y ácido piroglutámico favorece síntesis de nuevo glutatión reducido incrementando pool total, y provisión de cofactores que participan en generación de NADPH incluyendo benfotiamina que favorece vía de pentosas fosfato que genera NADPH respalda capacidad de glutatión reductasa de regenerar glutatión reducido desde forma oxidada manteniendo ratio apropiado.
¿Sabías que el alcohol inhibe secreción de hormona antidiurética por neurohipófisis mediante efectos sobre osmorreceptores hipotalámicos, generando diuresis que puede exceder volumen de líquido consumido en bebidas alcohólicas?
La hormona antidiurética, también llamada vasopresina, es liberada por neurohipófisis en respuesta a incrementos en osmolaridad plasmática detectados por osmorreceptores en hipotálamo, y actúa sobre túbulos colectores renales incrementando expresión de acuaporinas que son canales de agua en membrana apical que permiten reabsorción de agua libre desde orina en formación de vuelta a sangre. El alcohol suprime secreción de hormona antidiurética mediante mecanismos que incluyen efectos directos sobre osmorreceptores y posiblemente mediante efectos sobre neuronas que sintetizan hormona, resultando en reducción de expresión de acuaporinas y reducción en reabsorción de agua en túbulos colectores. Esta diuresis osmótica genera excreción de volumen de orina que puede exceder volumen de líquido consumido en bebidas alcohólicas particularmente cuando concentración de alcohol en bebidas es elevada, estableciendo balance neto negativo de líquidos que contribuye a deshidratación. La deshidratación reduce volumen plasmático incrementando concentración de metabolitos de alcohol y otros solutos, reduce perfusión cerebral que puede contribuir a cefalea mediante hipoxia relativa de tejido cerebral y activación de nociceptores perivasculares, y compromete función renal de excreción de metabolitos de alcohol y otros productos de desecho. La repleción de líquidos mediante consumo de agua antes, durante y después de consumo de alcohol es crítica para prevención de deshidratación, y consumo de electrolitos particularmente sodio y potasio que son también excretados en orina durante diuresis favorece mantenimiento de balance apropiado de fluidos y electrolitos. La rehidratación al día siguiente debe considerar que restauración completa de balance de líquidos puede requerir veinticuatro a cuarenta y ocho horas dependiendo de severidad de deshidratación y de función renal que regula conservación versus excreción de agua.
¿Sabías que la benfotiamina puede modular vía de hexosamina y vía de diacilglicerol-proteína quinasa C que son activadas durante hiperglucemia y estrés metabólico mediante desviación de metabolitos a vía de pentosas fosfato?
Durante hiperglucemia o estrés metabólico, incremento en concentración de intermediarios glucolíticos activa vías metabólicas alternativas incluyendo vía de hexosamina donde fructosa-6-fosfato es convertida a glucosamina-6-fosfato que es precursor de UDP-N-acetilglucosamina utilizada en glicosilación de proteínas, y vía de diacilglicerol donde gliceraldehído-3-fosfato es reducido a glicerol-3-fosfato que participa en síntesis de diacilglicerol que activa proteína quinasa C. La activación excesiva de estas vías puede contribuir a efectos adversos mediante glicosilación inadecuada de proteínas que modifica función, y activación de PKC que fosforila múltiples proteínas diana alterando señalización celular. La benfotiamina mediante provisión de tiamina pirofosfato activa transcetolasa que es enzima de vía de pentosas fosfato que convierte fructosa-6-fosfato y gliceraldehído-3-fosfato en xilulosa-5-fosfato y eritrosa-4-fosfato, desviando estos intermediarios desde vías que generan productos de glicación y activan PKC hacia vía que genera NADPH y ribosa-5-fosfato. Esta desviación metabólica puede reducir acumulación de productos finales de glicación avanzada que son formados mediante reacción no enzimática de azúcares con grupos amino de proteínas generando modificaciones que alteran estructura y función, y que son incrementados durante estrés metabólico. Durante metabolismo de alcohol donde perturbación metabólica por NADH elevado puede generar acumulación de intermediarios glucolíticos, activación de transcetolasa por benfotiamina puede favorecer procesamiento de estos intermediarios mediante vía que no genera productos tóxicos. Adicionalmente, NADPH generado por vía de pentosas fosfato es cofactor de glutatión reductasa que regenera glutatión reducido, estableciendo que desviación hacia vía de pentosas fosfato no solo reduce activación de vías que generan productos adversos sino que también favorece capacidad antioxidante.
¿Sabías que el NACET puede atravesar barrera hematoencefálica más eficientemente que N-acetilcisteína permitiendo provisión de precursores de glutatión directamente a neuronas y células gliales?
La barrera hematoencefálica es estructura altamente selectiva formada por células endoteliales de capilares cerebrales que están conectadas por uniones estrechas que previenen paso paracelular de moléculas, estableciendo que solo moléculas lipofílicas pequeñas o moléculas con transportadores específicos pueden entrar a cerebro desde circulación sistémica. La N-acetilcisteína es molécula cargada negativamente que tiene permeabilidad limitada a través de barrera hematoencefálica requiriendo transportadores que están expresados en niveles bajos en endotelio cerebral, limitando entrada a tejido cerebral. El NACET mediante esterificación de grupo carboxilo incrementa lipofilicidad permitiendo partición en bicapa lipídica de membranas endoteliales y atravesamiento mediante difusión pasiva sin dependencia en transportadores. Una vez en tejido cerebral, NACET es hidrolizado por esterasas presentes en neuronas y células gliales liberando N-acetilcisteína que proporciona cisteína para síntesis de glutatión. El cerebro tiene capacidad limitada de síntesis de glutatión de novo y depende parcialmente de importación de precursores desde circulación, haciendo que provisión eficiente de cisteína mediante NACET puede incrementar pools de glutatión cerebral. Durante consumo de alcohol, etanol y acetaldehído atraviesan barrera hematoencefálica y generan estrés oxidativo en tejido cerebral mediante mecanismos similares a efectos en hígado, y glutatión cerebral es consumido en neutralización de especies reactivas. La protección de neuronas contra estrés oxidativo es crítica dado que neuronas tienen capacidad limitada de regeneración comparado con hepatocitos, y daño acumulativo puede comprometer función neurológica a largo plazo. La provisión de precursores de glutatión mediante NACET que accede eficientemente a tejido cerebral establece soporte a capacidad antioxidante neuronal que complementa protección hepática.
¿Sabías que diferentes poblaciones humanas exhiben frecuencias variables de polimorfismos en genes que codifican alcohol deshidrogenasa y aldehído deshidrogenasa, modulando dramáticamente capacidad metabólica y susceptibilidad a efectos adversos de alcohol?
El gen ADH1B que codifica isoforma beta de alcohol deshidrogenasa tiene variantes incluyendo ADH1B2 que es común en poblaciones del este asiático con frecuencia de setenta a ochenta por ciento, y que codifica enzima con actividad catalítica aproximadamente cuarenta veces más elevada que variante ADH1B1 que es predominante en poblaciones europeas. Los individuos con ADH1B2 metabolizan etanol a acetaldehído mucho más rápidamente generando acumulación de acetaldehído que produce rubor facial, taquicardia y náusea. El gen ALDH2 que codifica aldehído deshidrogenasa mitocondrial tiene variante ALDH22 que es también común en poblaciones del este asiático con frecuencia de treinta a cincuenta por ciento, y que codifica enzima con actividad reducida en noventa por ciento aproximadamente debido a sustitución de glutamato por lisina en posición que es crítica para unión de NAD+. Los individuos heterocigotos para ALDH2*2 tienen actividad de aldehído deshidrogenasa reducida sustancialmente resultando en metabolismo lento de acetaldehído y acumulación pronunciada que genera manifestaciones adversas severas incluso con consumo mínimo de alcohol, mientras homocigotos tienen actividad casi nula estableciendo intolerancia completa. Estas variantes genéticas han sido propuestas como protectoras contra desarrollo de consumo problemático de alcohol dado que manifestaciones adversas desagradables actúan como disuasivo contra consumo, ilustrando que factores genéticos modulan no solo metabolismo sino también patrones conductuales de consumo. La comprensión de genotipo individual puede informar expectativas sobre respuesta metabólica a alcohol y sobre efectividad potencial de suplementación que modula metabolismo, dado que individuos con metabolismo rápido de etanol pero lento de acetaldehído pueden beneficiarse particularmente de componentes que favorecen actividad de aldehído deshidrogenasa como vitaminas del complejo B.
¿Sabías que el alcohol compromete absorción intestinal de múltiples vitaminas y minerales mediante efectos sobre integridad de mucosa intestinal, expresión de transportadores y función pancreática?
El consumo crónico de alcohol daña mucosa intestinal mediante múltiples mecanismos incluyendo generación de especies reactivas que causan peroxidación lipídica de membranas de enterocitos, alteración de uniones estrechas que incrementa permeabilidad permitiendo translocación de bacterias y componentes bacterianos que activan inflamación, y compromiso de renovación de epitelio que normalmente ocurre cada tres a cinco días mediante reducción de proliferación de células madre en criptas intestinales. Este daño compromete expresión y función de transportadores de nutrientes incluyendo transportadores de tiamina, folato, vitamina B12 con factor intrínseco, y minerales divalentes como zinc y magnesio, reduciendo absorción incluso cuando ingesta dietética es apropiada. El alcohol también compromete función pancreática mediante efectos tóxicos directos sobre células acinares que sintetizan enzimas digestivas, reduciendo secreción de lipasa que digiere grasas, amilasa que digiere carbohidratos complejos, y proteasas que digieren proteínas, estableciendo que digestión de macronutrientes es comprometida resultando en malabsorción de vitaminas liposolubles que requieren digestión de grasas para emulsificación y absorción, y de aminoácidos que son precursores de síntesis de glutatión y otros compuestos. El alcohol también reduce secreción de bicarbonato por páncreas que neutraliza acidez gástrica en duodeno estableciendo pH apropiado para actividad de enzimas pancreáticas, haciendo que incluso cuando enzimas son secretadas apropiadamente función puede ser comprometida por pH subóptimo. La suplementación con vitaminas del complejo B en formas bioactivas que no requieren modificación enzimática, y provisión de precursores de glutatión en formas que atraviesan membranas eficientemente como NACET, puede compensar parcialmente por absorción comprometida aunque optimización de integridad intestinal mediante reducción de consumo de alcohol, alimentación equilibrada y potencialmente mediante probióticos que restauran microbiota saludable es necesaria para corrección completa de malabsorción.
¿Sabías que los compuestos del jengibre pueden modular expresión de Nrf2 que es factor de transcripción maestro regulando expresión coordinada de más de doscientos genes que codifican enzimas antioxidantes y de detoxificación?
El Nrf2, factor nuclear eritroide 2 relacionado con factor 2, es factor de transcripción que en condiciones basales está secuestrado en citoplasma por proteína Keap1 que marca Nrf2 para degradación proteasomal manteniendo niveles bajos. Durante estrés oxidativo o exposición a electrófilos, cisteínas sensibles en Keap1 son modificadas alterando conformación y liberando Nrf2 que transloca a núcleo donde se une a elementos de respuesta antioxidante en promotores de genes diana activando transcripción. Los genes regulados por Nrf2 incluyen superóxido dismutasas que neutralizan radicales superóxido, catalasa que neutraliza peróxido de hidrógeno, glutatión peroxidasas y glutatión S-transferasas que neutralizan peróxidos y conjugan electrófilos, hemo oxigenasa-1 que degrada hemo generando biliverdina que tiene actividad antioxidante, y enzimas que sintetizan glutatión incluyendo gamma-glutamil-cisteína ligasa que cataliza paso limitante. Los gingeroles y shogaoles actúan como inductores de Nrf2 mediante modificación de cisteínas de Keap1 o mediante generación de especies reactivas leves que actúan como señal activando vía, estableciendo respuesta hormética donde exposición a estrés leve induce adaptaciones que incrementan resistencia a estrés mayor subsecuente. Durante metabolismo de alcohol donde generación de especies reactivas puede exceder capacidad basal de sistemas antioxidantes, inducción de expresión de enzimas antioxidantes mediante activación de Nrf2 incrementa capacidad total de neutralización. Sin embargo, inducción de expresión génica requiere horas para síntesis de nuevas proteínas haciendo que efectos son desarrollados gradualmente más que inmediatamente, estableciendo que activación de Nrf2 proporciona protección que se desarrolla durante uso sostenido más que protección aguda durante episodio individual de consumo de alcohol. La combinación de activación de Nrf2 que incrementa capacidad antioxidante endógena con provisión de precursores de glutatión que incrementan pools de sustrato para enzimas antioxidantes establece aproximación complementaria donde capacidad y sustrato son optimizados simultáneamente.
¿Sabías que el alcohol incrementa permeabilidad intestinal permitiendo translocación de endotoxinas bacterianas desde lumen intestinal a circulación portal que activan células de Kupffer en hígado generando respuesta inflamatoria?
La barrera intestinal está formada por monocapa de enterocitos conectados por uniones estrechas que son complejos proteicos incluyendo claudinas, ocludinas y proteínas de zonula occludens que sellan espacio entre células previniendo paso paracelular de macromoléculas, bacterias y componentes bacterianos desde lumen intestinal a circulación. El alcohol compromete integridad de uniones estrechas mediante múltiples mecanismos incluyendo fosforilación de proteínas de unión que altera ensamblaje, generación de especies reactivas que causan daño oxidativo a proteínas de unión, y modulación de expresión de claudinas específicas que determinan selectividad de uniones. El incremento en permeabilidad permite translocación de lipopolisacárido que es componente de membrana externa de bacterias gram-negativas y que actúa como potente activador de sistema inmune mediante unión a receptor TLR4 en células inmunes. Las endotoxinas que alcanzan hígado vía circulación portal son reconocidas por células de Kupffer que son macrófagos residentes en sinusoides hepáticos, activándolas para producir citoquinas proinflamatorias incluyendo TNF-alfa, IL-1 y IL-6 que activan células estrelladas hepáticas promoviendo producción de colágeno, y que generan respuesta de fase aguda sistémica. La activación crónica de células de Kupffer durante consumo repetido de alcohol contribuye a inflamación hepática persistente que puede comprometer función hepatocitaria y favorecer fibrogénesis. Los componentes antiinflamatorios en fórmula incluyendo gingeroles que inhiben NF-kappaB reduciendo producción de citoquinas, y dihidromiricetina que modula respuesta inflamatoria, pueden atenuar activación de células de Kupffer por endotoxinas. Adicionalmente, mantenimiento de integridad de barrera intestinal mediante alimentación que proporciona glutamina que es combustible preferido de enterocitos, probióticos que modulan microbiota favoreciendo especies que no generan endotoxinas masivamente, y reducción de consumo de alcohol que permite regeneración de epitelio intestinal, son estrategias complementarias para reducción de translocación de endotoxinas.
Momento estratégico de administración en relación a consumo de alcohol
La efectividad del Protector Anti-Alcohol depende críticamente de sincronización entre administración de fórmula y consumo de alcohol, dado que componentes deben alcanzar niveles circulantes y tisulares apropiados antes o durante periodo cuando metabolismo de etanol genera acetaldehído y especies reactivas que consumen glutatión y activan vías de estrés oxidativo e inflamación. Para uso preventivo óptimo, administre dos a tres cápsulas treinta a sesenta minutos antes de primer consumo de bebida alcohólica, permitiendo tiempo suficiente para absorción intestinal de componentes hidrosolubles como vitaminas del complejo B que son absorbidas rápidamente mediante transportadores específicos en yeyuno, y componentes lipofílicos como benfotiamina y NACET que requieren emulsificación por sales biliares y formación de micelas para absorción. Si consumo de alcohol se extiende durante más de tres a cuatro horas como en eventos sociales prolongados, considere administración de dosis adicional de dos cápsulas aproximadamente a mitad de periodo de consumo para mantener niveles de componentes que son metabolizados y eliminados durante exposición prolongada, particularmente relevante para NACET que es hidrolizado por esterasas tisulares y vitaminas B hidrosolubles que son excretadas cuando concentraciones plasmáticas exceden capacidad de reabsorción tubular renal. La administración post-consumo de dos a tres cápsulas antes de acostamiento o tan pronto como sea práctico después de último consumo de alcohol es crítica dado que metabolismo de alcohol residual continúa durante seis a ocho horas subsecuentes mientras etanol y acetaldehído permanecen en circulación, periodo durante el cual provisión de precursores de glutatión y cofactores enzimáticos respalda procesamiento continuo sin depleción de sustratos. Evite administración simultánea con grandes cantidades de alimentos muy grasos que pueden retrasar significativamente vaciamiento gástrico y absorción, aunque alimento moderado es apropiado para reducir probabilidad de molestia gástrica particularmente en individuos con sensibilidad digestiva incrementada.
Moderación consciente del consumo de alcohol
Aunque Protector Anti-Alcohol proporciona soporte metabólico durante procesamiento de etanol y metabolitos, la estrategia más efectiva para minimización de efectos adversos asociados con alcohol es moderación de cantidad y frecuencia de consumo dentro de límites que no saturan completamente capacidad de detoxificación hepática independientemente de suplementación. Limite consumo a cantidades moderadas definidas generalmente como no más de una bebida estándar por hora permitiendo que metabolismo hepático de alcohol que procede a velocidad relativamente constante de aproximadamente siete a diez gramos de etanol por hora en adulto promedio pueda procesar alcohol sin acumulación masiva de acetaldehído, aunque tasa metabólica individual varía sustancialmente debido a polimorfismos genéticos en alcohol deshidrogenasa y aldehído deshidrogenasa que pueden incrementar o reducir velocidad de oxidación. Establezca límite superior de consumo total por ocasión que considera masa corporal, sexo que influye en distribución de agua corporal y actividad de alcohol deshidrogenasa gástrica que es típicamente menor en mujeres, y tolerancia individual observada en experiencias previas, evitando consumo que genera intoxicación severa donde función cognitiva y motora es significativamente comprometida indicando que concentración sanguínea de alcohol excede capacidad de sistemas neurológicos de compensar efectos depresores sobre neurotransmisión. Alterne bebidas alcohólicas con agua u otras bebidas no alcohólicas en ratio de uno a uno que enlentece velocidad de consumo de alcohol proporcionando tiempo para metabolismo, y que mantiene hidratación dado que alcohol tiene efectos diuréticos mediante inhibición de hormona antidiurética incrementando pérdidas urinarias de líquidos que contribuyen a deshidratación que exacerba manifestaciones adversas. Evite combinación de alcohol con sustancias depresoras adicionales del sistema nervioso central incluyendo benzodiacepinas, opioides o antihistamínicos sedantes que potencian efectos depresores mediante mecanismos aditivos o sinérgicos incrementando riesgo de depresión respiratoria, y evite combinación con estimulantes incluyendo cafeína en dosis elevadas o sustancias ilícitas que enmascaran percepción de intoxicación permitiendo consumo excesivo de alcohol sin reconocimiento apropiado de nivel de intoxicación. Reconozca que suplementación no elimina completamente efectos de alcohol sobre juicio, coordinación motora y tiempo de reacción que comprometen capacidad de conducir vehículos o operar maquinaria, y que planificación de transporte alternativo es necesaria cuando consumo de alcohol ocurre.
Optimización nutricional antes, durante y después de consumo de alcohol
La alimentación estratégica antes, durante y después de consumo de alcohol modula absorción de etanol, proporciona sustratos para metabolismo y detoxificación, y favorece recuperación de homeostasis metabólica. Consuma comida sustancial que incluye proteínas de alta calidad, grasas saludables y carbohidratos complejos treinta a sesenta minutos antes de iniciar consumo de alcohol que enlentece vaciamiento gástrico y absorción de etanol reduciendo velocidad de incremento en concentración sanguínea de alcohol y permitiendo que metabolismo hepático de primer paso procese porción de alcohol antes de que alcance circulación sistémica, aunque efecto de metabolismo de primer paso es limitado dado que la mayoría de alcohol es absorbido en intestino delgado donde no hay metabolismo significativo. Las proteínas proporcionan aminoácidos incluyendo cisteína, glicina y glutamato que son precursores de glutatión, mientras grasas enlentecen tránsito gastrointestinal y carbohidratos complejos proporcionan glucosa que mantiene homeostasis glucémica durante periodo cuando metabolismo de alcohol genera NADH elevado que inhibe gluconeogénesis favoreciendo hipoglucemia particularmente en individuos que han ayunado previamente. Durante consumo de alcohol, continúe ingesta de alimentos priorizando opciones que proporcionan nutrientes densos más que alimentos procesados ricos en calorías vacías, incluyendo vegetales que proporcionan antioxidantes dietéticos incluyendo vitamina C, carotenoides y polifenoles que complementan sistemas antioxidantes endógenos, frutos secos que proporcionan vitamina E que protege lípidos de membranas de peroxidación, y frutas que proporcionan fructosa que puede modular ligeramente metabolismo de etanol aunque mecanismo y relevancia clínica son debatidos. Al día siguiente tras consumo de alcohol, consuma desayuno equilibrado que incluye proteínas para regeneración de proteínas hepáticas que pueden ser catabolizadas durante metabolismo de alcohol, carbohidratos para repleción de glucógeno hepático que es depletado cuando gluconeogénesis es inhibida, y frutas y vegetales que proporcionan electrolitos incluyendo potasio que puede ser depletado por efectos diuréticos de alcohol, y antioxidantes que continúan neutralizando especies reactivas residuales. Considere suplementación con Minerales Esenciales de Nootrópicos Perú que proporciona espectro completo de minerales traza y macrominerales incluyendo magnesio que es cofactor de enzimas que participan en metabolismo energético y puede ser depletado por excreción urinaria incrementada durante consumo de alcohol, zinc que participa en función de alcohol deshidrogenasa y puede ser movilizado desde reservas tisulares durante metabolismo intenso, y selenio que es componente de glutatión peroxidasas que neutralizan peróxidos generados durante estrés oxidativo asociado con metabolismo de etanol.
• Priorizar proteínas de alta calidad incluyendo pescado, aves, huevos y legumbres que proporcionan aminoácidos azufrados precursores de glutatión
• Incluir vegetales crucíferos como brócoli, col rizada y coles de Bruselas que contienen sulforafano que induce expresión de enzimas de fase II de detoxificación
• Consumir fuentes de vitamina C como cítricos, kiwi y pimientos que regeneran vitamina E oxidada y actúan como cofactor de reacciones de hidroxilación
• Incorporar alimentos ricos en colina como huevos y soja que proporcionan precursor de fosfatidilcolina que es fosfolípido mayoritario en membranas hepatocitarias
Hidratación estratégica y repleción de electrolitos
La hidratación apropiada antes, durante y después de consumo de alcohol es crítica para minimización de manifestaciones adversas dado que alcohol tiene efectos diuréticos potentes mediante inhibición de secreción de hormona antidiurética por neurohipófisis, incrementando excreción urinaria de agua libre que genera deshidratación que contribuye a cefalea, fatiga y función cognitiva comprometida mediante reducción en volumen plasmático, perfusión cerebral reducida, y concentración incrementada de metabolitos en tejidos. Consuma al menos dos a tres vasos de agua treinta a sesenta minutos antes de iniciar consumo de alcohol estableciendo estado de hidratación apropiado, y alterne cada bebida alcohólica con vaso de agua de tamaño similar durante consumo manteniendo balance de fluidos a pesar de pérdidas urinarias incrementadas, aproximación que también enlentece velocidad de consumo de alcohol proporcionando tiempo para metabolismo. Antes de acostamiento tras consumo de alcohol, consuma al menos dos a tres vasos adicionales de agua que compensan pérdidas acumuladas durante periodo de consumo y durante horas nocturnas cuando pérdidas insensibles por respiración y sudoración continúan sin repleción consciente, aunque evite consumo excesivo que genera necesidad de micción frecuente durante noche comprometiendo calidad de sueño. Al despertar, rehidrate con al menos dos vasos de agua inmediatamente y continúe consumo regular de líquidos durante día con objetivo de al menos dos a tres litros totales considerando pérdidas incrementadas del día previo. Considere inclusión de electrolitos en líquidos de rehidratación particularmente sodio y potasio que son excretados en orina y pueden ser depletados durante consumo prolongado de alcohol, mediante consumo de caldos que proporcionan sodio, agua de coco que proporciona potasio, o soluciones de rehidratación oral que contienen balance de electrolitos en concentraciones optimizadas para absorción intestinal. Evite rehidratación exclusivamente con bebidas que contienen cafeína en cantidades elevadas como café fuerte o bebidas energéticas dado que cafeína tiene efectos diuréticos leves que pueden exacerbar deshidratación, aunque cantidades moderadas de café o té son aceptables cuando combinadas con agua abundante. La calidad de agua es relevante particularmente en regiones donde agua de grifo contiene contaminantes o minerales en concentraciones que pueden comprometer función digestiva, prefiriendo agua filtrada o embotellada que proporciona hidratación sin carga adicional de compuestos que requieren procesamiento hepático.
Priorización de sueño reparador y recuperación
Aunque alcohol puede facilitar inicio de sueño mediante efectos depresores sobre sistema nervioso central que reducen latencia de sueño, compromete arquitectura y calidad de sueño mediante múltiples mecanismos incluyendo supresión de sueño REM que es fase donde consolidación de memorias y procesamiento emocional ocurren, fragmentación de sueño con despertares frecuentes durante segunda mitad de noche conforme alcohol es metabolizado y efectos sedantes disminuyen, y reducción en sueño profundo de ondas lentas que es fase donde secreción de hormona de crecimiento y reparación tisular son maximizadas. Priorice duración apropiada de sueño de siete a nueve horas tras consumo de alcohol reconociendo que calidad puede ser subóptima requiriendo duración extendida para obtener cantidad equivalente de sueño reparador, y establezca ambiente de sueño óptimo incluyendo temperatura fresca de dieciocho a veinte grados Celsius que favorece iniciación de sueño, oscuridad completa mediante cortinas opacas o máscara de sueño que previene supresión de melatonina por luz ambiental, y silencio o ruido blanco que enmascara sonidos disruptivos. Evite uso de dispositivos electrónicos que emiten luz azul durante hora previa a acostamiento que suprime secreción de melatonina mediante efectos sobre células ganglionares retinales intrínsecamente fotosensibles que proyectan a núcleo supraquiasmático regulando reloj circadiano, aunque filtros de luz azul o aplicaciones que modifican temperatura de color de pantallas pueden mitigar parcialmente efectos. Si sueño es significativamente comprometido tras consumo de alcohol con despertares frecuentes o sensación de sueño no reparador, considere siesta breve de veinte a treinta minutos durante día siguiente que proporciona recuperación parcial sin interferir con capacidad de iniciar sueño nocturno subsecuente, evitando siestas prolongadas de más de sesenta minutos que pueden generar inercia de sueño con sensación de aturdimiento al despertar y comprometer sueño nocturno. Reconozca que recuperación completa de déficit de sueño y restauración de homeostasis metabólica tras consumo significativo de alcohol puede requerir dos a tres días de sueño de calidad apropiada, y que consumo frecuente de alcohol que compromete sueño crónicamente genera deuda de sueño acumulativa que compromete función cognitiva, regulación emocional, función inmune y metabolismo durante periodos prolongados incluso cuando manifestaciones agudas de consumo de alcohol han resuelto.
Moderación de actividad física durante periodo de recuperación
Aunque actividad física regular es componente importante de estilo de vida saludable que favorece función cardiovascular, metabolismo y regulación de estrés, ejercicio intenso durante veinticuatro a cuarenta y ocho horas después de consumo significativo de alcohol puede exacerbar deshidratación, comprometer termorregulación, y incrementar demandas metabólicas en contexto donde homeostasis glucémica y función hepática aún se están recuperando. Limite ejercicio durante día siguiente a consumo de alcohol a actividad ligera a moderada incluyendo caminata, estiramiento suave o yoga que promueve circulación sin generar estrés cardiovascular o metabólico excesivo, evitando ejercicio de alta intensidad incluyendo entrenamiento de intervalos de alta intensidad o levantamiento de pesas pesadas que incrementan frecuencia cardíaca sustancialmente, generan producción de lactato que puede acumularse cuando metabolismo de lactato es comprometido por NADH elevado residual, y incrementan generación de especies reactivas de oxígeno en músculo esquelético que puede exacerbar estrés oxidativo cuando capacidad antioxidante aún se está recuperando. Si ejercicio es realizado durante periodo de recuperación, asegure hidratación incrementada antes, durante y después de actividad para compensar pérdidas por sudoración en contexto de deshidratación basal, consumiendo al menos quinientos mililitros de agua adicionales por cada treinta minutos de ejercicio moderado. Monitorice frecuencia cardíaca durante ejercicio notando si está elevada en relación a esfuerzo percibido que puede indicar compromiso de regulación cardiovascular por deshidratación o alteraciones electrolíticas, y reduzca intensidad o discontinúe actividad si experimenta mareo, cefalea severa, náusea o palpitaciones irregulares que pueden indicar respuesta cardiovascular inadecuada. Retome entrenamiento de intensidad normal solo cuando hidratación es completamente restaurada, sueño de calidad apropiada ha sido obtenido, y función cognitiva y física han retornado a niveles basales, típicamente requiriendo cuarenta y ocho a setenta y dos horas después de consumo significativo de alcohol dependiendo de cantidad consumida y capacidad individual de recuperación.
Complementación estratégica con cofactores sinérgicos
La efectividad del Protector Anti-Alcohol puede ser optimizada mediante suplementación complementaria con cofactores adicionales que participan en rutas metabólicas relacionadas con detoxificación, protección antioxidante y función hepática. El ácido alfa-lipoico es antioxidante anfipático que neutraliza especies reactivas en compartimentos acuosos y lipídicos, regenera vitamina C y vitamina E oxidadas extendiendo capacidad antioxidante, y participa como cofactor en complejos multienzimáticos mitocondriales incluyendo piruvato deshidrogenasa que convierte piruvato en acetil-CoA que puede ser comprometida durante metabolismo de alcohol por acumulación de NADH, considere suplementación con trescientos a seiscientos miligramos de ácido alfa-lipoico diariamente durante periodos de consumo regular de alcohol. La silimarina extraída de Silybum marianum modula función hepática mediante efectos antioxidantes, antiinflamatorios y potencialmente mediante estimulación de síntesis proteica en hepatocitos favoreciendo regeneración, y puede modular transportadores que median captación hepática y excreción biliar de compuestos, considere extracto estandarizado que proporciona doscientos a cuatrocientos miligramos de silimarina diariamente. El Complejo de Vitamina C con Camu Camu de Nootrópicos Perú proporciona ácido ascórbico junto con bioflavonoides y fitoquímicos de fuente natural que actúan sinérgicamente, regenerando vitamina E oxidada durante neutralización de radicales lipoperoxilo y actuando como cofactor de enzimas que participan en síntesis de colágeno que mantiene integridad de matriz extracelular hepática, considere mil a dos mil miligramos distribuidos durante día. La taurina es aminoácido condicional que conjuga ácidos biliares facilitando emulsificación de lípidos, actúa como osmoregulador manteniendo volumen celular, y tiene efectos citoprotectores en hepatocitos mediante modulación de homeostasis de calcio y estrés oxidativo, considere uno a dos gramos diarios particularmente durante periodos de consumo frecuente de alcohol. La L-carnitina transporta ácidos grasos de cadena larga a mitocondrias para beta-oxidación y puede actuar como buffer de grupos acilo previniendo acumulación de acil-CoA que inhibe enzimas metabólicas, considere quinientos a mil miligramos particularmente si metabolismo lipídico es comprometido durante consumo crónico de alcohol que favorece acumulación de lípidos en hepatocitos. Mantenga separación temporal apropiada entre diferentes suplementos considerando interacciones potenciales, administrando Protector Anti-Alcohol según protocolo de timing en relación a consumo de alcohol, y suplementos complementarios en horarios separados que optimizan absorción y minimizan competencia por transportadores o efectos sobre pH gástrico que pueden modular biodisponibilidad.
Monitorización de respuesta individual y ajuste de protocolo
La efectividad del Protector Anti-Alcohol y necesidad de ajustes en dosificación o protocolo varía sustancialmente entre individuos debido a polimorfismos genéticos que afectan metabolismo de alcohol y componentes de fórmula, masa corporal que determina volumen de distribución, función hepática basal que determina capacidad de detoxificación, y factores de estilo de vida incluyendo alimentación, hidratación y sueño que modulan recuperación. Establezca línea basal antes de inicio de uso de fórmula documentando manifestaciones típicas experimentadas tras consumo de alcohol incluyendo intensidad de cefalea, fatiga, compromiso cognitivo, manifestaciones gastrointestinales y duración total de periodo de recuperación, proporcionando referencia para evaluación de efectividad de suplementación. Durante primeros usos de fórmula, experimente con timing de administración incluyendo dosis preventiva treinta versus sesenta minutos antes de consumo, inclusión o exclusión de dosis durante consumo, y timing de dosis post-consumo inmediatamente tras último consumo versus antes de acostamiento, identificando protocolo que genera mejor respuesta según experiencia individual. Observe si dosificación de dos versus tres cápsulas por administración genera diferencias en efectividad, considerando incremento a tres cápsulas si dos es insuficiente o si consumo de alcohol es elevado, o mantenimiento de dos cápsulas si efectividad es apropiada minimizando ingesta de componentes. Documente cualquier manifestación adversa incluyendo molestia gástrica, náusea o cambios en evacuaciones que pueden indicar sensibilidad a componentes específicos o dosis excesiva, ajustando mediante reducción de dosis, administración con alimentos más sustanciales, o división de dosis en tomas más espaciadas. Evalúe efectividad no solo basándose en intensidad de manifestaciones inmediatas sino también en recuperación de función cognitiva y física, calidad de sueño tras consumo, y capacidad de retomar actividades normales durante día siguiente, reconociendo que objetivos pueden variar entre individuos donde algunos priorizan minimización de cefalea mientras otros priorizan función cognitiva o capacidad de ejercicio. Reconozca que efectividad puede variar según tipo de bebida alcohólica consumida dado que diferentes bebidas contienen congéneres variables que son compuestos adicionales generados durante fermentación que contribuyen a efectos adversos, y según contexto de consumo incluyendo presencia o ausencia de alimentos, velocidad de consumo, y factores ambientales como temperatura y altitud que modulan metabolismo y efectos de alcohol. Mantenga flexibilidad en protocolo ajustando basándose en experiencia acumulada más que adherencia rígida a dosificación específica, y reconozca que aunque optimización de protocolo puede mejorar experiencia, ninguna suplementación elimina completamente efectos de alcohol ni compensa por consumo excesivo que excede capacidad de detoxificación hepática.
Experiencia durante consumo activo de alcohol
Durante uso preventivo donde fórmula es administrada treinta a sesenta minutos antes de consumo de alcohol, algunos individuos reportan modulación de experiencia subjetiva que puede incluir transición más suave entre estados de sobriedad e intoxicación reflejando efectos de dihidromiricetina sobre receptores GABA-A, y reducción en intensidad de manifestaciones gastrointestinales incluyendo náusea o malestar epigástrico que pueden ocurrir durante consumo particularmente cuando alcohol es consumido sin alimentos, atribuible a efectos del extracto de jengibre sobre motilidad gástrica y receptores serotoninérgicos que median náusea. La provisión de cofactores vitamínicos y precursores de glutatión antes de exposición a alcohol establece que sistemas de detoxificación operan con disponibilidad optimizada de sustratos cuando metabolismo de etanol comienza, aunque cambios durante consumo activo son sutiles dado que metabolismo de alcohol genera carga metabólica sustancial que no puede ser completamente compensada por suplementación. La hidratación apropiada con alternancia de agua entre bebidas alcohólicas y consumo de alimentos que enlentecen absorción de etanol son estrategias complementarias que modulan experiencia durante consumo más significativamente que suplementación sola. Algunos individuos pueden no percibir diferencias evidentes durante consumo activo pero experimentan cambios más notables durante periodo de recuperación al día siguiente, estableciendo que timing de evaluación de efectos es relevante.
Recuperación durante primeras horas post-consumo
Durante periodo de seis a doce horas después de último consumo de alcohol, particularmente durante noche cuando sueño ocurre, metabolismo residual de etanol y acetaldehído continúa mientras fórmula administrada en dosis post-consumo proporciona soporte a procesamiento. Algunos individuos reportan calidad de sueño menos comprometida comparado con experiencias previas sin suplementación, reflejando potencialmente modulación de arquitectura de sueño mediante efectos combinados de magnesio en formas que atraviesan barrera hematoencefálica favoreciendo relajación, y protección de función neuronal mediante glutatión generado desde NACET que neutraliza especies reactivas en tejido cerebral. Al despertar, manifestaciones comunes asociadas con consumo de alcohol incluyendo cefalea cuya intensidad puede ser modulada mediante hidratación optimizada y reducción de inflamación por gingeroles, fatiga que puede ser menos pronunciada cuando función mitocondrial es protegida por antioxidantes, y compromiso cognitivo incluyendo dificultad de concentración o velocidad de procesamiento reducida pueden presentar intensidad variable dependiendo de cantidad de alcohol consumida y factores individuales. La experiencia es altamente variable entre individuos reflejando polimorfismos genéticos en enzimas que metabolizan alcohol y componentes de fórmula, masa corporal, función hepática basal y adherencia a estrategias complementarias incluyendo hidratación y alimentación apropiadas.
Adaptación durante primeras semanas de uso regular
Para individuos que consumen alcohol con frecuencia de tres o más días semanales y utilizan fórmula como soporte metabólico hepático mediante administración de dos cápsulas diarias independiente de timing de consumo de alcohol, la adaptación durante primeras dos a cuatro semanas puede incluir cambios sutiles en energía basal y función digestiva conforme homeostasis redox es optimizada y expresión de enzimas de detoxificación es modulada mediante activación de Nrf2 por extracto de jengibre. Algunos individuos experimentan cambios transitorios en consistencia o frecuencia de evacuaciones durante primera semana reflejando modulación de motilidad intestinal por electrolitos y adaptación de microbiota, manifestaciones que típicamente se normalizan con uso continuado. La tolerancia digestiva es generalmente apropiada dado que formas queladas y bioactivas de componentes presentan absorción mejorada con menor irritación gástrica, aunque administración con alimentos es recomendable para minimizar probabilidad de molestia particularmente en individuos con sensibilidad gástrica. Durante esta fase adaptativa, establecimiento de rutina consistente de administración mediante integración con actividades diarias como preparación de café matutino o comida principal favorece adherencia que es crítica para efectividad. La evaluación de respuesta debe considerar no solo intensidad de manifestaciones tras consumo de alcohol sino también parámetros como calidad de sueño, energía durante día y capacidad de mantener actividades normales al día siguiente de consumo.
Consolidación de efectos con uso sostenido (4-8 semanas)
Durante segundo y tercer mes de uso consistente, consolidación de efectos ocurre mediante repleción completa de reservas tisulares de cofactores vitamínicos que pueden estar depletadas durante consumo regular de alcohol, expresión sostenida de enzimas antioxidantes y de detoxificación inducidas mediante activación de Nrf2, y adaptaciones metabólicas que optimizan procesamiento de alcohol. Algunos individuos reportan que capacidad de recuperación tras consumo de alcohol mejora gradualmente donde duración de periodo con manifestaciones adversas es reducida y intensidad de compromiso funcional es menor, reflejando homeostasis metabólica optimizada que permite procesamiento más eficiente de alcohol y metabolitos. La función hepática basal puede ser favorecida mediante protección continua contra estrés oxidativo y modulación de inflamación, aunque evaluación objetiva mediante marcadores bioquímicos requiere análisis apropiados que están fuera del alcance de autoevaluación. Durante esta fase, algunos individuos experimentan que pueden tolerar cantidades similares de alcohol con menos manifestaciones adversas, aunque esto no debe interpretarse como licencia para incremento de consumo dado que daño acumulativo de alcohol ocurre independientemente de presencia o ausencia de manifestaciones agudas, y que objetivo de suplementación es soporte a homeostasis metabólica más que facilitación de consumo incrementado. La integración de suplementación con moderación consciente de consumo, hidratación apropiada y alimentación equilibrada establece aproximación integral donde suplementación complementa pero no reemplaza estrategias conductuales fundamentales.
Mantenimiento y uso a largo plazo (3-6 meses)
Tras tres a seis meses de uso consistente con implementación de ciclos que incluyen ocho a doce semanas de administración seguidas de pausas de siete a diez días, adaptaciones establecidas se mantienen estableciendo homeostasis metabólica optimizada que persiste durante pausas reflejando que mejoras no dependen exclusivamente de provisión exógena continua sino que incluyen adaptaciones sostenidas en expresión génica y función celular. Durante pausas, observación de parámetros como energía, calidad de sueño y recuperación tras consumo de alcohol proporciona retroalimentación sobre dependencia de mejoras en suplementación activa versus establecimiento de adaptaciones independientes, informando decisiones sobre continuación de uso. El uso a largo plazo es generalmente apropiado cuando consumo de alcohol es regular y cuando beneficios percibidos justifican continuación, aunque reevaluación periódica de necesidad es prudente considerando que objetivo último debe ser optimización de función mediante combinación de suplementación, moderación de consumo de alcohol y hábitos de estilo de vida saludables. Algunos individuos utilizan fórmula exclusivamente de manera preventiva y post-consumo durante eventos específicos de consumo de alcohol más que como suplementación diaria continua, aproximación que es válida aunque efectos sobre expresión de enzimas y repleción de reservas tisulares son menos pronunciados comparado con uso sostenido. La monitorización de función hepática mediante análisis bioquímicos periódicos puede ser prudente para individuos con consumo frecuente de alcohol independientemente de suplementación, proporcionando evaluación objetiva de status hepático que complementa observación subjetiva de manifestaciones.
Limitaciones y expectativas realistas
La efectividad del Protector Anti-Alcohol está fundamentalmente limitada por cantidad y frecuencia de consumo de alcohol donde ninguna suplementación puede compensar completamente por consumo excesivo que satura capacidad de detoxificación hepática generando acumulación de acetaldehído y estrés oxidativo que excede capacidad de neutralización independientemente de provisión de cofactores. La variabilidad individual en respuesta a suplementación es sustancial reflejando polimorfismos genéticos que afectan metabolismo de alcohol donde individuos con variantes de aldehído deshidrogenasa con actividad reducida experimentan acumulación pronunciada de acetaldehído que genera manifestaciones severas que pueden ser solo parcialmente moduladas por suplementación, y polimorfismos que afectan absorción y metabolismo de componentes de fórmula. Los factores de estilo de vida incluyendo calidad de alimentación que proporciona precursores endógenos de glutatión y cofactores vitamínicos desde fuentes dietéticas, hidratación que facilita excreción de metabolitos y mantiene perfusión tisular, sueño de calidad apropiada que permite recuperación y regeneración celular, y manejo de estrés que modula función inmune y respuesta inflamatoria influyen significativamente en efectividad de suplementación estableciendo que aproximación integral es necesaria. Esta fórmula no debe interpretarse como tratamiento para condiciones asociadas con consumo de alcohol ni como estrategia para facilitación de consumo incrementado, sino como soporte metabólico que complementa moderación consciente y hábitos saludables. Las expectativas deben ser realistas reconociendo que suplementación proporciona optimización de capacidad metabólica basal pero no elimina completamente efectos de alcohol sobre múltiples sistemas fisiológicos.
Fase de adaptación inicial
Durante primeros tres a siete días de uso, el organismo implementa ajustes homeostáticos adaptándose a provisión incrementada de cofactores vitamínicos, precursores de glutatión y compuestos bioactivos. Algunos individuos experimentan cambios transitorios en función digestiva incluyendo modificaciones leves en consistencia de evacuaciones o frecuencia que reflejan modulación de motilidad intestinal por extracto de jengibre y ajustes en microbiota a componentes de fórmula, manifestaciones que típicamente se resuelven durante segunda semana de uso. La administración con alimentos sustanciales que incluyen proteínas y grasas favorece tolerancia digestiva reduciendo probabilidad de náusea leve o malestar epigástrico que puede ocurrir con administración en ayunas particularmente durante fase adaptativa. Si experimenta molestia gástrica persistente, considere reducción temporal a una cápsula diaria durante semana adicional permitiendo adaptación gradual antes de progresar a dosis estándar, o división de dosis diaria en tomas muy espaciadas maximizando separación temporal. Algunos individuos pueden experimentar cambios sutiles en energía o estado de alerta durante primeros días reflejando optimización de metabolismo energético mediante cofactores vitamínicos, aunque estos cambios son típicamente sutiles más que dramáticos. Las manifestaciones que son severas, que persisten más allá de dos semanas, o que incluyen signos de hipersensibilidad como urticaria, hinchazón facial o dificultad respiratoria requieren discontinuación inmediata y evaluación apropiada, aunque reacciones de este tipo son raras con componentes en esta fórmula.
Compromiso requerido para resultados óptimos
La efectividad del Protector Anti-Alcohol depende críticamente de consistencia en administración y adherencia a protocolo de timing que sincroniza suplementación con consumo de alcohol para optimización de disponibilidad de cofactores cuando demanda metabólica es incrementada. Para uso preventivo y post-consumo durante eventos específicos de consumo de alcohol, administración de dos a tres cápsulas treinta a sesenta minutos antes de primer consumo y dos a tres cápsulas antes de acostamiento tras último consumo establece protocolo mínimo, con posibilidad de dosis adicional durante consumo prolongado que se extiende más de cuatro horas. Para uso como soporte metabólico hepático en contexto de consumo regular de alcohol, administración de dos cápsulas diarias con comida principal durante ciclos de ocho a doce semanas seguidos de pausas de siete a diez días establece patrón que optimiza repleción de reservas tisulares y expresión de enzimas de detoxificación mientras previene acumulación excesiva. La integración de suplementación con estrategias conductuales fundamentales incluyendo moderación de cantidad de alcohol consumida limitando a no más de una bebida estándar por hora, alternancia de bebidas alcohólicas con agua en ratio uno a uno, consumo de alimentos antes y durante ingesta de alcohol, y priorización de sueño de calidad apropiada tras consumo es esencial para maximización de efectividad. El compromiso también incluye monitorización de respuesta mediante observación de parámetros como intensidad y duración de manifestaciones tras consumo, calidad de sueño, energía y función cognitiva durante día siguiente, proporcionando retroalimentación para ajustes de protocolo y evaluación de efectividad individual que guía decisiones sobre continuación o modificación de uso.
Combinación específica de ingredientes
La fórmula de Protector Anti-Alcohol ha sido diseñada con una combinación única de ingredientes altamente biodisponibles y optimizados para garantizar una máxima absorción y eficacia. La integración de ingredientes como la dihidromiricetina (DHM), NACET, L-Ornitina HCL, y extracto de jengibre, en las dosis correctas, permite que el cuerpo reciba el soporte necesario para protegerse y recuperarse del estrés causado por el consumo de alcohol. La proporción exacta de cada ingrediente asegura que sus efectos sean sinérgicos, potenciando los beneficios para una acción más rápida y eficaz.
Efectividad superior
Lo que hace especial a Protector Anti-Alcohol es su capacidad para proporcionar resultados más rápidos y duraderos en comparación con fórmulas tradicionales. La combinación precisa de sus ingredientes no solo reduce los efectos inmediatos del alcohol, sino que también apoya la regeneración celular y la función hepática a largo plazo. La sinergia entre los componentes de la fórmula trabaja en conjunto para acelerar la desintoxicación y promover una recuperación óptima, lo que da como resultado menos incomodidad tras el consumo de alcohol. Además, la fórmula ofrece una ventaja significativa frente a otras en el mercado, que suelen centrarse en un solo ingrediente o en efectos limitados.
Beneficios específicos
Este complejo ha sido desarrollado con el propósito de abordar problemas concretos asociados con el consumo de alcohol, tales como el malestar estomacal, la fatiga y la deshidratación. Al ofrecer múltiples beneficios en uno, Protector Anti-Alcohol no solo combate los efectos inmediatos de la ingesta de alcohol, sino que también apoya la función hepática y la regeneración celular, optimizando el proceso de detoxificación del cuerpo. La combinación de vitaminas B, antioxidantes, y péptidos contribuye a mejorar la tolerancia y reducir el daño celular, asegurando resultados respaldados por la sinergia de ingredientes científicamente comprobados.
Conveniencia para el usuario
La dosificación de Protector Anti-Alcohol es práctica y fácil de seguir: solo se necesita tomar 3 cápsulas con agua después de consumir alcohol, lo que facilita su incorporación en la rutina diaria sin complicaciones. La fórmula está diseñada para ser bien tolerada por la mayoría de las personas, lo que reduce el riesgo de efectos secundarios comunes en otras soluciones. Gracias a su formato en cápsulas y su dosificación optimizada, este producto proporciona una forma conveniente de abordar los efectos negativos del alcohol de manera eficaz, sin tener que preocuparse por complicados regímenes de dosificación o tiempos estrictos de consumo.
Optimización nutricional
Para potenciar los efectos de Protector Anti-Alcohol, es importante seguir una dieta equilibrada y rica en nutrientes que favorezcan la absorción y los beneficios de la fórmula. Nutrientes como el magnesio, zinc y vitamina C son esenciales para el funcionamiento óptimo de los antioxidantes presentes en la fórmula, ayudando a potenciar la desintoxicación y la reparación celular. Consumir alimentos ricos en estas vitaminas y minerales, como frutas, vegetales de hojas verdes, frutos secos y semillas, apoyará de manera efectiva la absorción y maximizará los resultados. También se recomienda evitar el consumo excesivo de alimentos procesados, grasas trans y azúcar refinado, ya que pueden interferir en los beneficios del suplemento.
Hábitos de estilo de vida
El estilo de vida juega un papel fundamental en la eficacia de Protector Anti-Alcohol. Mantener patrones de sueño adecuados, con al menos 7-8 horas de descanso reparador, es clave para apoyar la regeneración celular y optimizar la respuesta del organismo al suplemento. Manejar el estrés mediante técnicas como la meditación o el yoga también mejora la efectividad, ya que reduce la inflamación y apoya la salud general del sistema. La importancia del descanso no puede subestimarse, ya que un cuerpo descansado y equilibrado responderá mejor al tratamiento. Establecer rutinas saludables para mejorar tanto el sueño como el manejo del estrés aumentará significativamente la eficacia de la fórmula.
Actividad física
Realizar actividad física moderada a intensa, como caminar, correr o entrenar con pesas, ayuda a acelerar el proceso de recuperación, mejora la circulación sanguínea y optimiza el metabolismo, lo que favorece la acción de Protector Anti-Alcohol. Se recomienda una frecuencia de 3-5 veces por semana para obtener los mejores resultados. Durante los entrenamientos, complementar con ejercicios cardiovasculares y de fuerza ayudará a maximizar el impacto de la fórmula en la salud general. Sincronizar el consumo del suplemento antes o después de los entrenamientos también puede ayudar a mejorar la tolerancia al alcohol y acelerar la recuperación del cuerpo tras su consumo.
Hidratación
La hidratación adecuada es esencial para potenciar los efectos de Protector Anti-Alcohol. Se recomienda consumir al menos 2-3 litros de agua al día, dependiendo de las necesidades personales y el nivel de actividad física. El agua de calidad, libre de contaminantes, es crucial para una hidratación eficiente y para mejorar la absorción de los nutrientes de la fórmula. Durante y después del consumo de alcohol, es aún más importante mantener una buena hidratación, ya que ayuda a reducir la deshidratación y mejora la función hepática. Estrategias como consumir agua con electrolitos también pueden ser beneficiosas para mantener el equilibrio de líquidos y optimizar los efectos de la fórmula.
Ciclo de suplementación
La consistencia es clave para obtener los mejores resultados de Protector Anti-Alcohol. Seguir el protocolo de dosificación recomendado y tomar el suplemento según los horarios indicados maximizará la absorción y los beneficios a largo plazo. Evitar los errores comunes, como saltarse dosis o alterar el horario de consumo, es crucial para mantener la eficacia del suplemento. Es importante seguir el protocolo con regularidad para obtener los efectos completos, y también se recomienda mantener la suplementación durante ciclos más largos para mejorar la tolerancia y protección frente a los efectos del alcohol.
Factores metabólicos
Optimizar el metabolismo es esencial para maximizar la efectividad de Protector Anti-Alcohol. Asegúrese de mantener un equilibrio hormonal adecuado y reducir los niveles de inflamación, lo que permitirá una mayor sensibilidad celular y una recuperación más rápida. Esto se puede lograr a través de la adopción de una dieta rica en antioxidantes, ejercicio regular y control del estrés. Al mejorar el metabolismo y la función celular, el cuerpo responderá de manera más eficiente al suplemento, lo que llevará a una protección más efectiva contra los efectos nocivos del alcohol.
Complementos sinérgicos
Para potenciar aún más los efectos de Protector Anti-Alcohol, se pueden considerar ciertos cofactores y suplementos sinérgicos. Por ejemplo, el magnesio y la vitamina C son complementos que pueden mejorar la biodisponibilidad de la fórmula, ayudando en la desintoxicación y recuperación celular. Otros complementos como el ácido alfa-lipoico o el silimarina (extracto de cardo mariano) pueden ser beneficiosos para apoyar la salud hepática y aumentar la capacidad de desintoxicación del cuerpo. Estas combinaciones potencian los efectos del suplemento y pueden mejorar la respuesta del cuerpo a la ingesta de alcohol.
Aspectos mentales
La mentalidad y las expectativas juegan un papel crucial en la efectividad de Protector Anti-Alcohol. Mantener una actitud positiva y gestionar adecuadamente el estrés son factores que pueden potenciar los resultados del suplemento. Practicar mindfulness o técnicas de relajación también puede reducir los efectos negativos del alcohol sobre la salud mental y física. Al enfocarse en un estilo de vida saludable y adoptar un enfoque equilibrado en cuanto a la tolerancia al alcohol, se mejoran tanto los resultados físicos como psicológicos del suplemento.
Personalización
Cada cuerpo responde de manera diferente, por lo que es importante adaptar el uso de Protector Anti-Alcohol a las necesidades personales. Escuchar las señales de su cuerpo, ajustar la dosis según la respuesta y ser flexible en el protocolo puede maximizar los beneficios. Cada persona puede tener un ritmo distinto en cuanto a los efectos del suplemento, por lo que es importante ser paciente y ajustar el enfoque según sea necesario, sin perder de vista los objetivos a largo plazo.
Soporte a detoxificación hepática y metabolismo de acetaldehído
• Ácido alfa-lipoico: Antioxidante anfipático que atraviesa compartimentos acuosos y lipídicos neutralizando especies reactivas generadas durante metabolismo de etanol por citocromo P450 2E1, y que actúa como cofactor de complejos multienzimáticos mitocondriales incluyendo piruvato deshidrogenasa que convierte piruvato en acetil-CoA durante procesamiento de acetato generado desde oxidación de acetaldehído. El ácido alfa-lipoico regenera vitamina C y vitamina E oxidadas extendiendo capacidad antioxidante establecida por dihidromiricetina y componentes del jengibre, y participa en regeneración de glutatión desde forma oxidada mediante modulación de expresión de gamma-glutamil-cisteína ligasa que cataliza paso limitante en síntesis de glutatión, estableciendo sinergia con NACET que proporciona cisteína como precursor limitante mientras ácido alfa-lipoico favorece expresión de maquinaria enzimática de síntesis.
• Silimarina: Flavonoide extraído de Silybum marianum que modula función hepatocitaria mediante efectos antioxidantes que neutralizan especies reactivas generadas durante metabolismo de alcohol, efectos antiinflamatorios mediante inhibición de NF-kappaB que reduce expresión de citoquinas proinflamatorias en células de Kupffer activadas por endotoxinas translocadas desde intestino, y potencialmente mediante estimulación de síntesis proteica en hepatocitos favoreciendo regeneración. La silimarina modula transportadores que median captación hepática y excreción biliar de compuestos estableciendo efectos sobre farmacocinética de metabolitos de alcohol, y actúa sinérgicamente con extracto de jengibre que también inhibe NF-kappaB estableciendo modulación dual de vías de señalización inflamatoria mediante mecanismos complementarios.
• Taurina: Aminoácido condicional que conjuga ácidos biliares facilitando emulsificación de lípidos y favoreciendo absorción de componentes lipofílicos de fórmula incluyendo benfotiamina y NACET, actúa como osmoregulador manteniendo volumen celular durante estrés osmótico generado por acumulación de metabolitos de alcohol, y tiene efectos citoprotectores en hepatocitos mediante modulación de homeostasis de calcio que previene activación de vías apoptóticas, y mediante neutralización de hipoclorito generado por mieloperoxidasa durante activación de neutrófilos que infiltran hígado durante respuesta inflamatoria. La taurina complementa efectos de L-ornitina en procesamiento de amonio dado que ambos aminoácidos participan en homeostasis de nitrógeno, estableciendo soporte dual a función hepática durante demanda metabólica incrementada por metabolismo de alcohol.
• Complejo de Vitamina C con Camu Camu: Proporciona ácido ascórbico junto con bioflavonoides y fitoquímicos de fuente natural que actúan sinérgicamente regenerando vitamina E oxidada durante neutralización de radicales lipoperoxilo que propagan peroxidación lipídica en membranas hepatocitarias, actuando como cofactor de enzimas que participan en síntesis de colágeno que mantiene integridad de matriz extracelular hepática, y favoreciendo absorción de componentes de fórmula mediante efectos sobre pH gástrico y modulación de transportadores intestinales. La vitamina C recicla dihidromiricetina oxidada durante actividad antioxidante extendiendo vida media funcional, y proporciona electrones para regeneración de glutatión desde forma oxidada mediante reducción no enzimática estableciendo complementariedad con provisión de precursores por NACET y ácido piroglutámico.
Optimización de homeostasis redox y protección antioxidante
• Vitamina D3 + K2: La vitamina D3 modula expresión de genes que codifican enzimas antioxidantes incluyendo glutatión peroxidasas y superóxido dismutasas mediante efectos sobre receptor de vitamina D que actúa como factor de transcripción, estableciendo sinergia con extracto de jengibre que activa Nrf2 que también regula expresión de enzimas antioxidantes mediante mecanismo complementario. La vitamina K2 participa en carboxilación de proteínas que contienen ácido gamma-carboxiglutámico incluyendo proteínas de matriz que previenen calcificación de tejidos blandos, y modula función mitocondrial mediante efectos sobre cadena respiratoria que pueden reducir generación de especies reactivas durante fosforilación oxidativa. La combinación con fórmula que contiene precursores de glutatión y antioxidantes directos establece protección multiestrato donde expresión de enzimas, provisión de cofactores y neutralización directa son optimizados coordinadamente.
• CoQ10 + PQQ: La coenzima Q10 actúa como transportador de electrones en cadena respiratoria mitocondrial transfiriendo electrones desde complejos I y II a complejo III, y en forma reducida ubiquinol neutraliza radicales lipoperoxilo en membranas mitocondriales previniendo peroxidación lipídica que compromete función de complejos respiratorios durante estrés oxidativo generado por metabolismo de alcohol. La pirroloquinolina quinona actúa como cofactor redox cíclico que puede aceptar y donar electrones múltiples veces sin ser consumida, y estimula biogénesis mitocondrial mediante activación de PGC-1alfa que coordina expresión de genes nucleares y mitocondriales que codifican proteínas mitocondriales. La combinación establece sinergia con benfotiamina que proporciona tiamina pirofosfato para enzimas mitocondriales y con NACET que proporciona glutatión para protección de mitocondrias, optimizando función mitocondrial mediante soporte a generación de energía, protección antioxidante y biogénesis.
• Metilfolato: Forma bioactiva de folato que participa con metilcobalamina en metionina sintasa que regenera metionina desde homocisteína, estableciendo sinergia directa dado que ambos cofactores son requeridos por misma enzima donde metilcobalamina es cofactor prostético mientras metilfolato es donador de grupo metilo. La regeneración de metionina mantiene pools de S-adenosilmetionina que es donador universal de grupos metilo en reacciones de metilación incluyendo síntesis de fosfatidilcolina que es fosfolípido mayoritario en membranas celulares cuya integridad es comprometida durante metabolismo de alcohol, y metilación de ADN que regula expresión génica. El metilfolato también regenera tetrahidrofolato que participa en síntesis de purinas y timidilato necesarios para replicación de ADN durante regeneración de hepatocitos, estableciendo que metilfolato complementa metilcobalamina no solo en reacción específica de metionina sintasa sino también en provisión de intermediarios para múltiples vías que requieren unidades de un carbono.
Soporte a función gastrointestinal y absorción
• L-Glutamina: Aminoácido que es combustible preferido de enterocitos proporcionando energía para mantenimiento de turnover epitelial que ocurre cada tres a cinco días y que es crítico para integridad de barrera intestinal comprometida durante consumo de alcohol. La glutamina participa en síntesis de glutatión como precursor de glutamato que es primer aminoácido incorporado en tripéptido, estableciendo sinergia con NACET que proporciona cisteína y con ácido piroglutámico que participa en ciclo gamma-glutamil, optimizando provisión de todos los precursores necesarios para síntesis de glutatión en enterocitos donde protección contra estrés oxidativo es crítica para mantenimiento de función de absorción. La glutamina también modula permeabilidad intestinal mediante efectos sobre expresión de proteínas de uniones estrechas previniendo translocación de endotoxinas que activan inflamación hepática.
• Probióticos de cepas específicas (Lactobacillus plantarum, Bifidobacterium longum): Modulan composición de microbiota intestinal favoreciendo especies que no generan endotoxinas masivamente y que producen ácidos grasos de cadena corta incluyendo butirato que es combustible para colonocitos y que tiene efectos antiinflamatorios mediante inhibición de NF-kappaB. Los probióticos mejoran integridad de barrera intestinal mediante producción de metabolitos que fortalecen uniones estrechas reduciendo translocación de lipopolisacárido que activa células de Kupffer, estableciendo sinergia con componentes antiinflamatorios de fórmula incluyendo gingeroles que actúan en hígado mientras probióticos actúan en intestino estableciendo protección coordinada. Los probióticos también pueden metabolizar componentes de fórmula modificando biodisponibilidad mediante desconjugación o conversión a metabolitos activos, aunque interacciones específicas con componentes de esta fórmula requieren caracterización.
• Zinc (Siete Zincs + Cobre): El zinc es cofactor de alcohol deshidrogenasa que cataliza oxidación de etanol a acetaldehído, estableciendo que disponibilidad de zinc modula directamente velocidad de metabolismo de alcohol aunque saturación de enzima con cofactor ocurre a concentraciones relativamente bajas haciendo que suplementación solo es relevante cuando status de zinc es subóptimo. El zinc participa en mantenimiento de integridad de barrera intestinal mediante efectos sobre expresión de proteínas de uniones estrechas y mediante función como cofactor de metaloproteasas que regulan renovación de matriz extracelular, complementando efectos de L-glutamina. La inclusión de cobre previene desbalance inducido por suplementación con zinc dado que ambos minerales compiten por absorción mediante transportador DMT1, y cobre participa en ceruloplasmina que oxida hierro facilitando transporte estableciendo función independiente relevante para homeostasis de metales.
Modulación de respuesta al estrés y recuperación
• L-Teanina: Aminoácido presente en té que modula neurotransmisión mediante incremento en síntesis de GABA que es neurotransmisor inhibitorio principal, y mediante modulación de receptores de glutamato reduciendo excitotoxicidad. La L-teanina establece sinergia con dihidromiricetina que modula receptores GABA-A contrarrestando efectos de etanol, donde DHM actúa durante exposición a alcohol mientras L-teanina proporciona soporte a neurotransmisión GABAérgica durante recuperación. La L-teanina también modula ondas cerebrales incrementando actividad alfa que se asocia con estado de relajación sin sedación, y puede favorecer calidad de sueño que es comprometida durante consumo de alcohol mediante supresión de sueño REM.
• Magnesio (Ocho Magnesios): Cofactor de más de trescientas enzimas incluyendo enzimas que participan en metabolismo energético, síntesis de proteínas y ácidos nucleicos, y función de bombas iónicas que mantienen gradientes electroquímicos a través de membranas celulares. El magnesio es excretado en cantidades incrementadas durante consumo de alcohol debido a efectos diuréticos de etanol, y depleción puede comprometer función neuromuscular, metabolismo energético y homeostasis cardiovascular. La provisión de múltiples formas de magnesio incluyendo formas queladas con absorción mejorada, formas que atraviesan barrera hematoencefálica como magnesio treonato, y formas con liberación sostenida establece repleción completa de pools tisulares. El magnesio actúa como antagonista de receptores NMDA que median neurotransmisión glutamatérgica excitadora, complementando efectos de L-teanina sobre sistema GABAérgico estableciendo modulación dual de excitabilidad neuronal.
• Glicina: Aminoácido que es neurotransmisor inhibitorio en médula espinal y tronco cerebral modulando procesamiento de información sensorial y función motora, y que es precursor de glutatión junto con glutamato y cisteína estableciendo sinergia con NACET que proporciona cisteína y ácido piroglutámico que proporciona glutamato. La glicina participa en conjugación de fase II en hígado mediante formación de conjugados glicina con ácidos orgánicos facilitando excreción, estableciendo función en detoxificación que complementa conjugación con glutatión. La glicina también modula receptores de glicina en sistema nervioso central que son distintos de sitio de glicina en receptores NMDA, y consumo de glicina antes de acostamiento puede favorecer calidad de sueño mediante mecanismos que incluyen modulación de temperatura corporal central que es regulada por hipotálamo y que es crítica para iniciación de sueño.
Optimización de biodisponibilidad y absorción
• Piperina: Alcaloide extraído de Piper nigrum que incrementa biodisponibilidad de múltiples nutracéuticos mediante inhibición de glucuronidación que es reacción de fase II que conjuga compuestos con ácido glucurónico facilitando excreción, mediante inhibición de CYP3A4 y otros citocromos P450 que metabolizan xenobióticos reduciendo metabolismo de primer paso, y mediante efectos sobre permeabilidad intestinal incrementando absorción. La piperina puede incrementar biodisponibilidad de componentes de esta fórmula incluyendo gingeroles y shogaoles del extracto de jengibre que son sustrato de glucuronidación, dihidromiricetina que es metabolizada por enzimas de fase II, y potencialmente vitaminas del complejo B mediante efectos sobre transportadores intestinales. La modulación de rutas de absorción y metabolismo establece que piperina actúa como cofactor potenciador transversal que optimiza aprovechamiento de múltiples componentes simultáneamente, aunque timing de administración debe considerar que inhibición de enzimas metabolizadoras puede también afectar metabolismo de otros compuestos incluyendo medicación prescrita requiriendo evaluación de compatibilidad cuando múltiples sustancias son consumidas.
¿Para qué sirve esta fórmula?
La Fórmula Protector Anti-Alcohol de Nootrópicos Perú integra complejo sinérgico de dihidromiricetina, precursores de glutatión, cofactores vitamínicos del complejo B en formas bioactivas, L-ornitina y extracto de jengibre estandarizado, diseñado para respaldar capacidad metabólica hepática de procesamiento de etanol y acetaldehído mediante soporte a sistemas de detoxificación de fase I y fase II que catalizan oxidación y conjugación de metabolitos de alcohol. La formulación favorece homeostasis redox celular mediante provisión de NACET que es precursor lipofílico de glutatión con biodisponibilidad incrementada comparado con N-acetilcisteína estándar, y ácido piroglutámico que participa en ciclo gamma-glutamil facilitando regeneración de glutatión desde productos de degradación. Los cofactores vitamínicos incluyendo benfotiamina que proporciona tiamina pirofosfato para enzimas que metabolizan acetato, piridoxal-5-fosfato que participa en transaminación de aminoácidos y síntesis de neurotransmisores, y metilcobalamina que participa en metabolismo de homocisteína aseguran que enzimas dependientes de vitaminas B operan apropiadamente durante demanda metabólica incrementada asociada con metabolismo de alcohol. La L-ornitina respalda ciclo de urea que procesa amonio generado durante catabolismo de aminoácidos que es incrementado cuando metabolismo de alcohol genera NADH elevado que inhibe gluconeogénesis, mientras extracto de jengibre modula inflamación mediante inhibición de ciclooxigenasa-2 y NF-kappaB, y favorece función gastrointestinal mediante efectos sobre motilidad y receptores que median náusea. Esta fórmula está diseñada para uso preventivo antes de consumo de alcohol, durante consumo prolongado, y post-consumo para respaldar procesamiento de alcohol residual, o como soporte metabólico hepático continuo en contexto de consumo regular de alcohol, complementando estrategias de moderación consciente, hidratación apropiada y alimentación equilibrada.
¿Puedo usar esta fórmula si consumo alcohol solo ocasionalmente?
El Protector Anti-Alcohol es apropiado tanto para uso ocasional sincronizado con eventos específicos de consumo de alcohol como para uso regular en contexto de consumo frecuente. Para individuos que consumen alcohol ocasionalmente con frecuencia menor a una vez por semana, el protocolo de dosificación preventiva y post-consumo proporciona soporte durante eventos específicos sin necesidad de administración diaria continua. Administre dos a tres cápsulas treinta a sesenta minutos antes de iniciar consumo de alcohol estableciendo disponibilidad de cofactores y precursores cuando metabolismo de etanol comienza, y dos a tres cápsulas antes de acostamiento tras último consumo proporcionando soporte a procesamiento de alcohol residual durante periodo nocturno cuando metabolismo continúa. Este protocolo de uso agudo es efectivo dado que componentes incluyendo dihidromiricetina que modula receptores GABA-A y actividad de enzimas que metabolizan alcohol, NACET que proporciona cisteína para síntesis de glutatión que es consumido durante conjugación de acetaldehído, y vitaminas del complejo B que actúan como cofactores de enzimas metabólicas exhiben efectos que se desarrollan dentro de horas después de administración más que requiriendo semanas de uso para establecimiento de efectos. Sin embargo, individuos que consumen alcohol ocasionalmente pero en cantidades sustanciales cuando consumen pueden beneficiarse de implementación de ciclo breve de uso diario durante semana previa a evento anticipado de consumo para optimización de reservas tisulares de glutatión y expresión de enzimas de detoxificación, aunque esta aproximación requiere planificación anticipada que puede no ser práctica para eventos no programados. La ventaja de uso ocasional es que evita necesidad de adherencia diaria continua reduciendo costo y complejidad de protocolo, aunque individuos con consumo regular de alcohol tres o más días semanales pueden beneficiarse más de administración diaria continua que mantiene homeostasis metabólica optimizada entre episodios de consumo.
¿Esta fórmula me permitirá beber más alcohol sin consecuencias?
La fórmula Protector Anti-Alcohol proporciona soporte metabólico a capacidad hepática de procesamiento de alcohol pero no elimina efectos de alcohol sobre sistema nervioso central, función cardiovascular, o capacidad de juicio y coordinación motora que son comprometidas durante intoxicación. El objetivo de suplementación es optimización de detoxificación de etanol y acetaldehído mediante provisión de cofactores y precursores que favorecen actividad de enzimas que metabolizan alcohol, y protección contra estrés oxidativo e inflamación generados durante metabolismo, no facilitación de consumo incrementado ni eliminación de riesgos asociados con intoxicación. Independientemente de suplementación, alcohol compromete función cognitiva incluyendo memoria, atención y toma de decisiones, altera coordinación motora y tiempo de reacción incrementando riesgo de accidentes, y genera intoxicación que puede ser peligrosa particularmente cuando concentración sanguínea de etanol alcanza niveles que comprometen función respiratoria o cardiovascular. La suplementación no modifica concentración sanguínea de alcohol de manera que permita conducir vehículos o operar maquinaria seguramente cuando alcohol ha sido consumido, y planificación de transporte alternativo es necesaria independientemente de uso de fórmula. Adicionalmente, consumo excesivo de alcohol genera daño acumulativo a múltiples órganos incluyendo hígado donde exposición crónica puede contribuir a acumulación de lípidos y activación de células estrelladas que producen colágeno, cerebro donde neurotoxicidad puede comprometer función cognitiva a largo plazo, y tracto gastrointestinal donde compromiso de integridad de mucosa favorece inflamación, independientemente de presencia o ausencia de manifestaciones agudas que pueden ser moduladas por suplementación. La aproximación apropiada es integración de suplementación con moderación consciente de cantidad y frecuencia de consumo dentro de límites que no saturan capacidad de detoxificación, estableciendo que suplementación complementa pero no reemplaza responsabilidad individual en decisiones sobre consumo de alcohol.
¿Cuánto tiempo antes de beber alcohol debo tomar la fórmula?
El timing óptimo para dosis preventiva es treinta a sesenta minutos antes de iniciar consumo de alcohol, permitiendo tiempo suficiente para absorción intestinal de componentes y distribución a tejidos incluyendo hígado donde metabolismo de etanol ocurre predominantemente. La absorción de componentes hidrosolubles incluyendo vitaminas del complejo B que son absorbidas mediante transportadores específicos en yeyuno ocurre relativamente rápido con niveles circulantes incrementados detectables dentro de treinta a cuarenta y cinco minutos, mientras componentes lipofílicos incluyendo benfotiamina y NACET que requieren emulsificación por sales biliares pueden requerir cuarenta y cinco a sesenta minutos para absorción óptima particularmente cuando administrados con alimentos que enlentecen vaciamiento gástrico pero favorecen secreción biliar. La dihidromiricetina alcanza concentraciones plasmáticas máximas aproximadamente una a dos horas después de administración oral según estudios farmacocinéticos limitados disponibles, estableciendo que administración sesenta minutos antes de consumo de alcohol establece niveles circulantes apropiados cuando exposición a etanol comienza. Si timing de consumo de alcohol es impredecible o si decisión de consumir alcohol es tomada espontáneamente sin planificación anticipada, administración inmediatamente antes de primer consumo aún proporciona soporte dado que metabolismo de alcohol continúa durante horas después de consumo y que componentes absorbidos durante consumo estarán disponibles cuando metabolismo es más intenso. Sin embargo, efectividad puede ser subóptima comparado con administración preventiva apropiada dado que establecimiento de niveles tisulares de cofactores requiere tiempo y que metabolismo inicial de alcohol puede ocurrir antes de que niveles óptimos sean alcanzados. Evite administración excesivamente temprana más de dos horas antes de consumo de alcohol dado que componentes con vida media relativamente corta incluyendo NACET pueden ser metabolizados y eliminados antes de que exposición a alcohol ocurra, reduciendo disponibilidad cuando demanda metabólica es máxima.
¿Puedo tomar esta fórmula con el estómago vacío?
La administración del Protector Anti-Alcohol con el estómago vacío es técnicamente posible dado que formas queladas y bioactivas de componentes presentan biodisponibilidad mejorada que no depende completamente de presencia de alimentos, aunque administración con alimentos proporciona ventajas que favorecen tolerancia digestiva y optimización de absorción de componentes específicos. La presencia de alimentos en estómago amortigua contacto directo de componentes concentrados con mucosa gástrica reduciendo probabilidad de náusea leve o malestar epigástrico que algunos individuos experimentan con administración en ayunas particularmente durante primeros usos cuando adaptación aún no ha ocurrido. Los alimentos que contienen grasas estimulan secreción de bilis que emulsifica componentes lipofílicos incluyendo benfotiamina y NACET facilitando formación de micelas que son absorbidas en yeyuno, mientras proteínas en alimentos pueden proporcionar aminoácidos que comparten transportadores con algunos componentes o que actúan como señales para secreción de enzimas digestivas y hormonas gastrointestinales que modulan motilidad. Sin embargo, para uso preventivo donde objetivo es alcanzar niveles circulantes elevados rápidamente antes de exposición a alcohol, administración sin alimentos o con alimento muy ligero puede ser preferible para maximizar velocidad de absorción estableciendo niveles pico más rápidamente, aunque este beneficio debe balancearse contra probabilidad incrementada de molestia gástrica en individuos con sensibilidad. Si experimenta náusea o malestar con administración en ayunas, cambie a administración con comida ligera que incluye al menos pequeña porción de proteína y grasa como yogur con nueces o tostada con aguacate que proporciona matriz sin ser comida completa sustancial que retrasa significativamente absorción. Para dosis post-consumo antes de acostamiento, administración con al menos dos vasos de agua es mínimo recomendable independientemente de presencia de alimentos dado que hidratación es crítica para compensar efectos diuréticos de alcohol, y alimento ligero puede ser apropiado aunque apetito puede ser reducido durante este periodo.
¿Esta fórmula es compatible con medicamentos de prescripción?
La compatibilidad del Protector Anti-Alcohol con medicación prescrita requiere evaluación caso por caso considerando clases específicas de medicamentos y mecanismos de interacción potenciales. Los componentes de fórmula pueden interactuar con medicación mediante competencia por enzimas metabolizadoras particularmente citocromos P450 que metabolizan múltiples fármacos, mediante modulación de transportadores que median absorción intestinal o excreción renal y biliar de medicamentos, o mediante efectos aditivos o antagónicos sobre sistemas fisiológicos que son también blanco de medicación. La dihidromiricetina es metabolizada por enzimas de fase II incluyendo glucuronosiltransferasas que también metabolizan múltiples fármacos, estableciendo potencial de competencia que puede modular niveles circulantes de medicación aunque evidencia específica de interacciones clínicamente significativas es limitada. El extracto de jengibre inhibe ciclooxigenasa-2 y puede modular agregación plaquetaria mediante efectos sobre producción de tromboxano, estableciendo consideración teórica para individuos que consumen anticoagulantes incluyendo warfarina o antiagregantes plaquetarios como clopidogrel, aunque dosis de gingeroles en esta fórmula es modesta y riesgo de interacciones significativas es probablemente bajo requiriendo precaución más que contraindicación absoluta. Las vitaminas del complejo B en dosis suplementales generalmente no interactúan significativamente con medicación común aunque administración simultánea con levodopa debe evitarse dado que piridoxina incrementa descarboxilación periférica de levodopa reduciendo llegada a sistema nervioso central, requiriendo separación temporal de al menos cuatro horas. Los individuos que consumen medicación múltiple particularmente inmunosupresores, antidiabéticos que modulan glucemia donde alcohol también tiene efectos hipoglucémicos potenciales, o medicación para tiroides deben mantener comunicación con prescriptor sobre suplementación proporcionando información completa sobre composición para evaluación de compatibilidad. Mantenga separación temporal de al menos dos horas entre medicación y suplemento como precaución general que minimiza interacciones por absorción competitiva, y monitorice respuesta a medicación durante primeras semanas de uso de fórmula observando si efectividad de medicación es modificada sugiriendo interacción que requiere ajuste de dosis o discontinuación de suplemento.
¿Puedo usar esta fórmula si tengo función hepática comprometida?
Los individuos con compromiso documentado de función hepática incluyendo elevación de transaminasas hepáticas, alteraciones en función sintética evidenciada por reducción en albúmina o factores de coagulación, o manifestaciones clínicas de insuficiencia hepática deben ejercer precaución con suplementación y consultar con hepatólogo o profesional que gestiona condición hepática antes de iniciar uso. El hígado es sitio primario de metabolismo de componentes de fórmula incluyendo dihidromiricetina que es conjugada con ácido glucurónico, NACET que es hidrolizado y metabolizado, y vitaminas del complejo B que son fosforiladas y participan en múltiples reacciones, estableciendo que función hepática comprometida puede alterar farmacocinética de componentes generando acumulación o metabolismo alterado. Adicionalmente, aunque objetivo de fórmula es soporte a función hepática durante metabolismo de alcohol, la presencia de compromiso hepático establecido modifica fundamentalmente respuesta metabólica a alcohol donde capacidad de detoxificación es reducida y riesgo de efectos adversos es incrementado sustancialmente, estableciendo que consumo de alcohol en contexto de enfermedad hepática es altamente desaconsejable independientemente de suplementación. Los componentes individuales incluyendo silimarina que es comúnmente utilizada en contexto de función hepática comprometida, y N-acetilcisteína que es utilizada clínicamente en casos de intoxicación por acetaminofeno que compromete función hepática sugieren que precursores de glutatión pueden ser beneficiosos, aunque dosis, forma de administración y monitorización apropiadas en contexto de enfermedad hepática establecida difieren de uso como suplemento preventivo en individuos con función hepática normal. Los individuos con historial de compromiso hepático que ha resuelto completamente con función normalizada pueden considerar uso de fórmula con monitorización periódica de función hepática mediante análisis bioquímicos que evalúan transaminasas, bilirrubina y función sintética, asegurando que suplementación no genera efectos adversos no anticipados. Crítico es reconocer que suplementación no es sustituto de abstinencia de alcohol que es recomendación fundamental para personas con compromiso hepático, y que uso de esta fórmula nunca debe interpretarse como facilitación de consumo seguro de alcohol en contexto de enfermedad hepática.
¿Cuántas cápsulas debo tomar si planeo beber una cantidad significativa de alcohol?
La dosificación apropiada debe considerar cantidad anticipada de alcohol, duración de periodo de consumo, y masa corporal individual, aunque es crítico reconocer que no existe dosis de suplementación que compense completamente por consumo excesivo de alcohol que satura capacidad de detoxificación hepática. Para consumo moderado definido como dos a cuatro bebidas estándar durante periodo de dos a cuatro horas, protocolo estándar de dos a tres cápsulas preventivas treinta a sesenta minutos antes de consumo y dos a tres cápsulas post-consumo antes de acostamiento es generalmente apropiado. Para consumo más extenso que se anticipa incluirá cuatro a seis bebidas durante periodo de cuatro a seis horas, considere dosis preventiva de tres cápsulas, dosis adicional de dos cápsulas aproximadamente a mitad de periodo de consumo para mantener niveles de componentes que son metabolizados durante exposición prolongada, y dosis post-consumo de tres cápsulas antes de acostamiento. Evite exceder dosis total de seis a ocho cápsulas en periodo de veinticuatro horas para prevenir ingesta excesiva de componentes individuales particularmente vitaminas del complejo B donde aunque límites superiores tolerables son elevados para la mayoría de vitaminas B, dosis muy elevadas pueden generar manifestaciones incluyendo neuropatía periférica con piridoxina en dosis superiores a doscientos miligramos diarios durante meses aunque riesgo con uso ocasional es bajo. Para individuos con masa corporal elevada superior a noventa a cien kilogramos, incremento proporcional de dosis a extremo superior de rango puede ser apropiado para compensar volumen de distribución incrementado, mientras individuos con masa corporal baja inferior a sesenta kilogramos pueden iniciar con extremo inferior de rango evaluando respuesta. Sin embargo, énfasis debe estar en moderación de cantidad de alcohol consumida más que en incremento de dosis de suplementación para compensar consumo excesivo, reconociendo que capacidad de detoxificación hepática tiene límites absolutos que no pueden ser extendidos indefinidamente mediante suplementación, y que daño acumulativo de alcohol ocurre independientemente de efectividad de suplementación en modulación de manifestaciones agudas.
¿Puedo combinar esta fórmula con otros suplementos?
La combinación del Protector Anti-Alcohol con otros suplementos es generalmente compatible aunque requiere consideración de composición de otros suplementos para prevenir duplicación excesiva de componentes o interacciones que pueden modular absorción o efectos. Si consume multivitamínico que contiene vitaminas del complejo B, verifique dosis de tiamina, piridoxina y cobalamina en multivitamínico y sume a contenido de Protector Anti-Alcohol para asegurar que ingesta total no excede límites superiores tolerables, aunque para la mayoría de vitaminas B estos límites son suficientemente elevados que exceso es improbable con suplementación típica. Si consume suplementos de minerales incluyendo zinc, magnesio o selenio que participan en función antioxidante y detoxificación, mantenga separación temporal de al menos dos horas entre Protector Anti-Alcohol y suplementos minerales para minimizar competencia por absorción mediante transportadores de metales divalentes compartidos. La combinación con suplementos complementarios incluyendo ácido alfa-lipoico que regenera otros antioxidantes, silimarina que modula función hepática, probióticos que mejoran integridad de barrera intestinal, o L-glutamina que es combustible de enterocitos puede proporcionar soporte adicional mediante mecanismos complementarios, aunque costo total y complejidad de protocolo deben considerarse evaluando si beneficios justifican administración de múltiples suplementos. Los suplementos que contienen estimulantes incluyendo cafeína en dosis elevadas deben utilizarse con precaución durante consumo de alcohol dado que efectos estimulantes pueden enmascarar percepción de nivel de intoxicación permitiendo consumo excesivo sin reconocimiento apropiado de compromiso de función cognitiva y motora. Evite combinación con suplementos que contienen kava, valeriana u otros compuestos con efectos sedantes que pueden potenciar efectos depresores de alcohol sobre sistema nervioso central incrementando riesgo de sedación excesiva o depresión respiratoria. Si consume múltiples suplementos regularmente, considere consulta con profesional de salud para revisión de protocolo completo evaluando compatibilidad, necesidad de cada componente, y optimización de timing de administración que minimiza interacciones mientras maximiza efectividad de componentes individuales.
¿Esta fórmula afectará mi capacidad de conducir después de beber?
La fórmula Protector Anti-Alcohol no modifica concentración sanguínea de etanol ni elimina efectos de alcohol sobre función cognitiva, coordinación motora, tiempo de reacción o juicio que son críticos para conducción segura de vehículos. Aunque suplementación puede modular algunos aspectos de metabolismo de alcohol mediante soporte a actividad de enzimas hepáticas que oxidan etanol a acetaldehído y acetaldehído a acetato, velocidad de metabolismo de alcohol tiene límite fijo determinado por cantidad de alcohol deshidrogenasa en hepatocitos que procesa aproximadamente siete a diez gramos de etanol por hora independientemente de suplementación. El alcohol compromete múltiples dominios de función neurológica incluyendo atención sostenida y dividida que es necesaria para monitorización simultánea de múltiples aspectos de ambiente de conducción, coordinación visuomotora que determina precisión de respuestas motoras a estímulos visuales, y función ejecutiva incluyendo inhibición de respuestas inapropiadas y toma de decisiones bajo presión temporal. La modulación de receptores GABA-A por dihidromiricetina que contrarresta algunos efectos de etanol sobre estos receptores según estudios preclínicos no debe interpretarse como restauración completa de función cognitiva y motora a niveles de sobriedad, y evidencia en humanos caracterizando efectos sobre parámetros de conducción es ausente. Independientemente de uso de suplementación, cualquier consumo de alcohol que resulta en concentración sanguínea de etanol por encima de límites legales que varían por jurisdicción pero típicamente son cincuenta a ochenta miligramos por decilitro para conducción regular establece compromiso de capacidad de conducción y riesgo legal. La única aproximación segura es planificación de transporte alternativo antes de consumo de alcohol incluyendo designación de conductor sobrio, uso de servicios de transporte compartido, o permanencia en ubicación donde consumo ocurre hasta que concentración sanguínea de alcohol retorna a cero mediante metabolismo que requiere múltiples horas dependiendo de cantidad consumida. La suplementación no debe generar falsa confianza en capacidad de conducir seguramente después de consumo de alcohol, y responsabilidad individual en decisiones sobre conducción después de beber no es modificada por uso de suplementos.
¿Puedo tomar esta fórmula durante embarazo o lactancia?
El uso del Protector Anti-Alcohol durante embarazo y lactancia se desaconseja debido a múltiples consideraciones incluyendo insuficiente evidencia de seguridad de componentes específicos en estas poblaciones, y fundamentalmente porque consumo de alcohol durante embarazo está contraindicado dado riesgo de efectos teratogénicos sobre desarrollo fetal incluyendo compromiso de desarrollo neurológico que puede resultar en déficits cognitivos y conductuales permanentes. No existe nivel de consumo de alcohol durante embarazo que ha sido establecido como completamente seguro, y recomendación universal de organismos de salud es abstinencia completa de alcohol durante gestación, estableciendo que uso de suplemento diseñado para soporte durante consumo de alcohol es fundamentalmente inapropiado en contexto de embarazo. Durante lactancia, alcohol pasa a leche materna alcanzando concentraciones similares a concentración sanguínea materna, y exposición de lactante a alcohol puede comprometer desarrollo neurológico y alterar patrones de sueño y alimentación, estableciendo que consumo de alcohol durante lactancia también es desaconsejable. Los componentes individuales de fórmula incluyendo vitaminas del complejo B son nutrientes esenciales durante embarazo y lactancia, pero dosis específicas en formulación suplemental y combinación con otros componentes incluyendo dihidromiricetina donde evidencia de seguridad en embarazo es ausente no han sido evaluadas sistemáticamente en estas poblaciones. Si está embarazada, planea embarazo, o está lactando, priorice abstinencia completa de alcohol que es recomendación fundamental para protección de desarrollo fetal y neonatal, y si tiene necesidad de suplementación con vitaminas del complejo B o precursores de glutatión por indicaciones específicas, consulte con obstetra o profesional de salud para recomendación de formulaciones diseñadas específicamente para embarazo y lactancia que han sido evaluadas para seguridad en estas poblaciones y que proporcionan dosis apropiadas de nutrientes sin componentes de seguridad no establecida.
¿Qué debo hacer si experimento efectos secundarios?
La tolerancia al Protector Anti-Alcohol es generalmente apropiada dado que formulación utiliza formas bioactivas y queladas de componentes con biodisponibilidad mejorada y tolerancia digestiva superior comparado con formas simples, aunque algunos individuos pueden experimentar manifestaciones transitorias particularmente durante primeros días de uso. Si experimenta molestia gástrica leve, náusea o malestar epigástrico, administre fórmula con alimentos sustanciales que incluyen proteínas y grasas que proporcionan matriz que amortigua contacto con mucosa gástrica, o considere reducción temporal de dosis a una o dos cápsulas diarias durante semana permitiendo adaptación gradual antes de progresar a dosis estándar. Los cambios transitorios en consistencia o frecuencia de evacuaciones que pueden ocurrir durante primeros días reflejando modulación de motilidad intestinal por extracto de jengibre típicamente se resuelven con uso continuado y no requieren intervención si no son severos, aunque si diarrea es significativa o persistente más allá de una semana considere reducción de dosis o discontinuación temporal. Si experimenta cefalea, activación inusual, o dificultad para iniciar sueño que pueden reflejar sensibilidad a componentes específicos, considere administración más temprana durante día evitando administración nocturna que puede interferir con sueño en individuos sensibles, o reducción de dosis. Las manifestaciones que sugieren hipersensibilidad incluyendo urticaria, prurito generalizado, hinchazón facial o labial, dificultad respiratoria o sibilancias requieren discontinuación inmediata de fórmula y evaluación médica apropiada dado que aunque reacciones alérgicas a componentes de esta fórmula son raras, pueden ocurrir en individuos con predisposición. Si experimenta manifestaciones severas que comprometen función diaria, manifestaciones que persisten más allá de dos semanas sin mejoría a pesar de ajustes de dosis y timing, o cualquier manifestación que genera preocupación significativa, discontinúe uso y considere evaluación profesional para determinación de causa y compatibilidad de fórmula con condiciones individuales. Documente manifestaciones específicas incluyendo timing en relación a administración, severidad, y duración que proporciona información útil para evaluación de causalidad y decisiones sobre reinicio con modificaciones o discontinuación permanente.
¿Puedo tomar esta fórmula si sigo una dieta vegetariana o vegana?
La compatibilidad del Protector Anti-Alcohol con alimentación vegetariana o vegana depende de composición específica de cápsulas que puede variar entre lotes o presentaciones. Verifique panel de ingredientes en etiqueta de producto para identificación de composición de cápsula donde gelatina que es derivada de colágeno animal típicamente de origen bovino o porcino indica que formulación no es apropiada para veganos y posiblemente no apropiada para vegetarianos dependiendo de restricciones específicas, mientras hidroxipropilmetilcelulosa que es polímero vegetal derivado de celulosa indica compatibilidad con alimentación vegetariana y vegana. Los componentes activos de fórmula incluyendo dihidromiricetina extraída de Hovenia dulcis, extracto de jengibre de Zingiber officinale, y L-ornitina que típicamente es producida mediante fermentación bacteriana son apropiados para vegetarianos y veganos, mientras vitaminas del complejo B pueden ser derivadas de fuentes sintéticas o de fermentación que son apropiadas, o en algunos casos de fuentes animales que no son apropiadas requiriendo verificación con fabricante si adherencia estricta es requerida. El NACET como derivado sintético de N-acetilcisteína es apropiado independientemente de fuente, mientras ácido piroglutámico puede ser derivado de fuentes vegetales o sintéticas. Los vegetarianos y veganos pueden tener riesgo incrementado de deficiencias de vitaminas del complejo B particularmente vitamina B12 que está ausente en alimentos vegetales no fortificados, haciendo que suplementación con formas bioactivas como metilcobalamina puede ser particularmente relevante en esta población. Si sigue alimentación vegetariana o vegana estricta y composición de cápsula no es apropiada, considere apertura de cápsulas y mezcla de contenido con alimentos o bebidas que enmascaran sabor, o contacte con fabricante para investigar disponibilidad de formulación en cápsulas vegetales. La alimentación basada en plantas bien planificada proporciona múltiples componentes que respaldan función hepática y homeostasis redox incluyendo antioxidantes de frutas y vegetales, aminoácidos de legumbres y granos, y grasas saludables de nueces y semillas, estableciendo que aunque suplementación puede proporcionar soporte adicional, alimentación equilibrada es fundamento de optimización de función metabólica.
¿Esta fórmula tiene interacciones con café o bebidas con cafeína?
La interacción entre Protector Anti-Alcohol y cafeína es compleja dado que ambos compuestos son metabolizados por enzimas hepáticas incluyendo citocromos P450, y dado que combinación de alcohol y cafeína genera efectos que deben considerarse independientemente de suplementación. La cafeína es metabolizada predominantemente por CYP1A2 mientras componentes de fórmula son metabolizados por múltiples isoformas incluyendo CYP2E1 para algunos compuestos, estableciendo que competencia directa por metabolismo es limitada aunque modulación de expresión de enzimas por un compuesto puede afectar metabolismo de otro. La combinación de alcohol con cafeína en dosis elevadas es problemática dado que efectos estimulantes de cafeína sobre sistema nervioso central pueden enmascarar percepción de nivel de intoxicación por alcohol que tiene efectos depresores, permitiendo que individuos consuman cantidades mayores de alcohol sin reconocimiento apropiado de compromiso de función cognitiva y motora estableciendo riesgo incrementado de intoxicación severa y toma de decisiones inadecuadas. Esta interacción entre alcohol y cafeína ocurre independientemente de uso de Protector Anti-Alcohol y no es modulada significativamente por suplementación, estableciendo que precaución con consumo simultáneo de alcohol y cafeína es recomendable independientemente. El consumo de café o té en cantidades moderadas con administración de fórmula fuera de contexto de consumo de alcohol es generalmente compatible sin interacciones significativas, aunque individuos con sensibilidad a cafeína pueden experimentar que combinación con componentes que modulan neurotransmisión incluyendo vitaminas del complejo B que participan en síntesis de neurotransmisores puede modular efectos de cafeína de manera sutil. Si consume bebidas con cafeína durante o después de consumo de alcohol, limite cantidad a niveles moderados evitando bebidas energéticas con contenido muy elevado de cafeína, mantenga hidratación apropiada con agua dado que tanto alcohol como cafeína tienen efectos diuréticos que pueden exacerbar deshidratación, y reconozca que presencia de cafeína no modifica concentración sanguínea de alcohol ni restaura capacidad de conducir seguramente después de beber.
¿Cuánto tiempo permanecen los efectos después de tomar la fórmula?
La duración de efectos del Protector Anti-Alcohol varía según componente específico dado que cada compuesto tiene farmacocinética distinta determinada por absorción, distribución, metabolismo y excreción. Las vitaminas del complejo B que son hidrosolubles alcanzan concentraciones plasmáticas máximas dentro de una a tres horas después de administración y son excretadas predominantemente en orina con vida media de varias horas, estableciendo que niveles elevados persisten durante aproximadamente cuatro a ocho horas después de administración aunque variabilidad individual es sustancial. El NACET es hidrolizado por esterasas tisulares liberando N-acetilcisteína que tiene vida media de aproximadamente dos a tres horas, estableciendo que efectos sobre provisión de cisteína para síntesis de glutatión son más pronunciados durante primeras cuatro a seis horas aunque glutatión sintetizado desde cisteína proporcionada persiste en células durante periodos más prolongados. La dihidromiricetina tiene vida media que no está completamente caracterizada en humanos aunque estudios preclínicos sugieren eliminación relativamente rápida dentro de varias horas, estableciendo que efectos sobre modulación de receptores GABA-A y metabolismo de alcohol son probablemente más pronunciados durante periodo de cuatro a ocho horas después de administración. Los gingeroles y shogaoles del extracto de jengibre son metabolizados mediante glucuronidación y sulfatación con vida media de varias horas, aunque metabolitos pueden persistir en circulación durante periodos más prolongados. Para uso preventivo y durante consumo de alcohol, efectos son más relevantes durante periodo de metabolismo activo de alcohol que se extiende durante seis a ocho horas después de último consumo dependiendo de cantidad, estableciendo que timing de administración debe considerar que pico de efectos de componentes debe coincidir con periodo de demanda metabólica máxima. Para uso como soporte metabólico hepático continuo mediante administración diaria, efectos acumulativos sobre expresión de enzimas de detoxificación y repleción de reservas tisulares de glutatión se desarrollan durante semanas y persisten durante días después de discontinuación, estableciendo que efectos sostenidos difieren de efectos agudos de dosis individual.
¿Puedo usar esta fórmula para recuperarme después de una noche de consumo excesivo?
El Protector Anti-Alcohol puede proporcionar soporte durante recuperación después de consumo de alcohol mediante provisión de precursores de glutatión que favorecen neutralización de especies reactivas residuales, cofactores vitamínicos que respaldan metabolismo energético y función de enzimas que procesan metabolitos de alcohol que aún están presentes, y extracto de jengibre que modula inflamación y función gastrointestinal. Si no administró dosis preventiva antes de consumo o dosis post-consumo inmediatamente después, administración al despertar de dos a tres cápsulas con agua abundante y alimento ligero si tolerado puede proporcionar soporte durante fase de recuperación, aunque efectividad es subóptima comparado con protocolo completo que incluye dosificación preventiva dado que daño oxidativo y depleción de glutatión ya han ocurrido durante noche cuando metabolismo de alcohol fue más intenso sin disponibilidad optimizada de cofactores y precursores. Durante recuperación, priorice hidratación mediante consumo de al menos dos a tres litros de agua distribuidos durante día para compensar deshidratación por efectos diuréticos de alcohol, consumo de electrolitos mediante caldos que proporcionan sodio o agua de coco que proporciona potasio, y alimentación equilibrada que incluye proteínas para regeneración de proteínas hepáticas y frutas y vegetales que proporcionan antioxidantes dietéticos y carbohidratos para repleción de glucógeno. El sueño adicional si posible proporciona recuperación dado que muchos procesos de reparación celular y consolidación de homeostasis metabólica ocurren durante sueño, aunque calidad de sueño inmediatamente después de consumo de alcohol puede ser comprometida requiriendo recuperación durante noches subsecuentes. Evite ejercicio intenso durante veinticuatro a cuarenta y ocho horas después de consumo significativo dado que demandas metabólicas de ejercicio combinadas con recuperación de metabolismo de alcohol pueden generar estrés excesivo, aunque actividad ligera como caminata favorece circulación sin generar carga sustancial. Reconozca que recuperación completa de consumo excesivo puede requerir cuarenta y ocho a setenta y dos horas dependiendo de cantidad consumida y capacidad individual de recuperación, y que suplementación proporciona soporte pero no acelera mágicamente procesos que requieren tiempo para normalización de homeostasis metabólica, regeneración de reservas depletadas y reparación de daño celular que ocurrió durante exposición.
¿Esta fórmula ayudará con la resaca al día siguiente?
La modulación de manifestaciones asociadas con consumo de alcohol durante día siguiente, comúnmente referidas como resaca, depende de múltiples factores incluyendo cantidad de alcohol consumida que determina carga metabólica, adherencia a protocolo de dosificación preventiva y post-consumo que optimiza disponibilidad de cofactores durante metabolismo, hidratación apropiada que minimiza deshidratación que contribuye significativamente a manifestaciones, y factores individuales incluyendo polimorfismos genéticos que afectan metabolismo de alcohol. El Protector Anti-Alcohol mediante soporte a detoxificación de acetaldehído que es metabolito altamente reactivo contribuyente a manifestaciones adversas, neutralización de especies reactivas que generan inflamación y comprometen función celular, y provisión de extracto de jengibre que modula inflamación y función gastrointestinal puede reducir intensidad de algunas manifestaciones en algunos individuos, aunque variabilidad en respuesta es sustancial y algunos individuos pueden experimentar beneficios pronunciados mientras otros experimentan modulación mínima. Las manifestaciones que pueden ser más susceptibles a modulación incluyen náusea y malestar gastrointestinal donde extracto de jengibre tiene efectos bien caracterizados sobre motilidad y receptores que median náusea, y posiblemente cefalea donde modulación de inflamación y mantenimiento de hidratación contribuyen aunque mecanismos de cefalea asociada con alcohol son complejos incluyendo vasodilatación, deshidratación y efectos sobre neurotransmisión. La fatiga y compromiso cognitivo pueden ser menos susceptibles a modulación dado que reflejan parcialmente déficit de sueño de calidad que no puede ser compensado completamente por suplementación, y efectos residuales de alcohol sobre función neurológica que persisten durante periodo de recuperación. Crítico es reconocer que ausencia de manifestaciones severas o reducción en intensidad de manifestaciones no indica que daño celular no ocurrió, dado que muchos efectos de alcohol sobre tejidos incluyendo estrés oxidativo, compromiso de síntesis proteica y alteración de homeostasis metabólica ocurren sin manifestaciones subjetivas necesariamente correlacionadas, estableciendo que minimización de manifestaciones no debe interpretarse como licencia para consumo incrementado. La aproximación óptima es uso de fórmula como componente de estrategia integral que incluye moderación de consumo, hidratación apropiada, alimentación equilibrada y sueño adecuado, más que como solución única para eliminación completa de manifestaciones que permite consumo sin consecuencias.
¿Necesito ciclar el uso de esta fórmula o puedo tomarla continuamente?
El patrón óptimo de uso depende de frecuencia de consumo de alcohol y objetivos individuales. Para individuos que consumen alcohol ocasionalmente con frecuencia menor a una vez por semana, uso exclusivo como dosificación preventiva y post-consumo sincronizada con eventos específicos de consumo sin administración diaria continua entre eventos es apropiado y no requiere implementación de ciclos formales dado que uso es inherentemente intermitente. Para individuos que consumen alcohol regularmente con frecuencia de tres o más días semanales y utilizan fórmula como soporte metabólico hepático continuo mediante administración diaria de dos cápsulas, implementación de ciclos con periodos de ocho a doce semanas de uso seguidos de pausas de siete a diez días es recomendable para evaluación de efectos sostenidos independientes de suplementación activa y para prevención de acumulación excesiva de componentes aunque riesgo con componentes en esta fórmula es bajo dado que vitaminas del complejo B son hidrosolubles y excretadas eficientemente, y otros componentes son metabolizados y eliminados sin acumulación sustancial. Las pausas permiten que mecanismos homeostáticos de regulación que pueden downregularse durante provisión exógena continua retornen a sensibilidad basal, aunque evidencia de que esta downregulación ocurre con componentes de esta fórmula es limitada haciendo que ciclado es precaución más que necesidad establecida. Durante pausas, mantenga alimentación equilibrada rica en precursores de glutatión desde fuentes dietéticas incluyendo proteínas que proporcionan aminoácidos azufrados, vegetales crucíferos que inducen expresión de enzimas de detoxificación, y fuentes de vitaminas del complejo B, y observe parámetros como energía, digestión y recuperación tras consumo de alcohol para evaluación de dependencia en suplementación. Si manifestaciones significativas retornan durante pausa sugiriendo que mejoras dependen completamente de suplementación activa, considere que uso prolongado continuo puede ser apropiado aunque evaluación de moderación de consumo de alcohol y optimización de factores de estilo de vida que influyen independientemente debe ser prioridad. El uso continuo durante años sin pausas es opción válida particularmente cuando consumo de alcohol es frecuente y cuando beneficios percibidos justifican continuación, aunque monitorización periódica mediante análisis bioquímicos de función hepática proporciona evaluación objetiva que complementa observación subjetiva.
¿Puedo abrir las cápsulas y mezclar el contenido con alimentos o bebidas?
Las cápsulas del Protector Anti-Alcohol pueden abrirse y contenido puede mezclarse con alimentos o bebidas si deglución de cápsulas completas es problemática, aunque esta modificación presenta consideraciones. El sabor de componentes cuando liberados directamente sin encapsulación puede ser perceptible y potencialmente desagradable particularmente dado contenido de extracto de jengibre que tiene sabor picante pronunciado, haciendo que mezcla con alimentos o bebidas que tienen sabor fuerte que enmascara sabor de componentes incluyendo yogur, smoothie con frutas, compota de manzana o jugo es recomendable. Consuma mezcla completa inmediatamente después de preparación para asegurar ingesta de dosis total y para minimizar exposición de componentes a aire que puede generar oxidación de compuestos sensibles aunque estabilidad de la mayoría de componentes en esta fórmula es apropiada a temperatura ambiente durante periodos breves. Evite mezcla con líquidos muy calientes que pueden degradar componentes sensibles a temperatura particularmente vitaminas aunque componentes en esta fórmula son relativamente estables a temperaturas de alimentos y bebidas normales. La mezcla con alimentos o bebidas ácidas incluyendo jugo de cítricos o vinagre no compromete estabilidad de componentes y puede facilitar solubilización de algunos compuestos. Si apertura de cápsulas es necesaria regularmente debido a dificultad de deglución, considere que integridad de formas queladas y bioactivas es mantenida cuando liberadas en ambiente intestinal independientemente de si liberación ocurre desde cápsula que se desintegra en estómago o desde mezcla con alimento que es consumida, estableciendo que biodisponibilidad no es comprometida significativamente por apertura de cápsulas. Sin embargo, timing de liberación puede ser ligeramente alterado dado que desintegración de cápsula en estómago proporciona liberación relativamente coordinada de todos los componentes, mientras mezcla con alimento puede generar liberación más gradual conforme alimento es digerido, aunque impacto sobre efectividad es probablemente mínimo para la mayoría de individuos.
- Este producto es un suplemento alimenticio diseñado para respaldar capacidad metabólica durante procesamiento de alcohol, y no debe utilizarse como sustituto de moderación consciente de consumo de alcohol ni como facilitación de consumo excesivo que compromete función hepática, neurológica y cardiovascular independientemente de suplementación.
- Mantenga el envase herméticamente cerrado en lugar fresco y seco, protegido de luz solar directa, humedad excesiva y fuentes de calor, a temperatura ambiente entre quince y veinticinco grados Celsius para preservar estabilidad de componentes bioactivos incluyendo dihidromiricetina y vitaminas del complejo B.
- No consumir si el sello de seguridad está roto o muestra signos de alteración, y verificar fecha de caducidad impresa en el envase antes de consumir para asegurar que componentes mantienen potencia apropiada.
- Mantener fuera del alcance de personas vulnerables que puedan consumir el producto inadecuadamente sin comprensión de propósito específico y protocolo de dosificación apropiado.
- Se desaconseja enfáticamente el uso durante embarazo dado que consumo de alcohol durante gestación está contraindicado por riesgo de efectos teratogénicos sobre desarrollo fetal incluyendo compromiso de desarrollo neurológico, estableciendo que suplemento diseñado para soporte durante consumo de alcohol es fundamentalmente inapropiado en esta población, y dado que evidencia de seguridad de componentes específicos incluyendo dihidromiricetina durante embarazo es insuficiente.
- Se desaconseja el uso durante lactancia dado que alcohol pasa a leche materna alcanzando concentraciones similares a concentración sanguínea materna y exposición de lactante puede comprometer desarrollo neurológico, estableciendo que consumo de alcohol durante lactancia es desaconsejable independientemente de suplementación, y dado que seguridad de componentes de fórmula durante lactancia no ha sido establecida mediante estudios controlados.
- Las personas con función hepática comprometida documentada mediante elevación de transaminasas, alteraciones en función sintética o manifestaciones clínicas de insuficiencia hepática deben ejercer precaución extrema reconociendo que consumo de alcohol en contexto de enfermedad hepática es altamente desaconsejable independientemente de suplementación, y que metabolismo de componentes de fórmula puede ser alterado por función hepática comprometida.
- Evitar el uso en personas con historial documentado de hipersensibilidad o reacciones alérgicas a componentes de formulación incluyendo extracto de jengibre de familia Zingiberaceae, dihidromiricetina extraída de Hovenia dulcis, o a excipientes de cápsulas incluyendo gelatina o hidroxipropilmetilcelulosa según composición específica.
- Las personas que consumen medicación prescrita incluyendo anticoagulantes donde extracto de jengibre puede tener interacción teórica mediante modulación de agregación plaquetaria, medicación metabolizada por citocromos P450 donde competencia por metabolismo puede alterar niveles de medicamento, o levodopa donde piridoxina incrementa descarboxilación periférica reduciendo efectividad deben mantener separación temporal de al menos dos horas y monitorizar respuesta a medicación durante primeras semanas de uso.
- Mantener separación temporal de al menos cuatro horas entre administración de este suplemento y medicamentos para tiroides incluyendo levotiroxina donde minerales y otros componentes pueden formar complejos reduciendo absorción hormonal, comprometiendo control de función tiroidea.
- Iniciar con dosis conservadora de una a dos cápsulas durante primer uso evaluando tolerancia digestiva particularmente en individuos con sensibilidad gástrica conocida o historial de intolerancia a suplementos, y progresar a dosis estándar de dos a tres cápsulas solo si tolerancia es apropiada sin manifestaciones significativas.
- Si experimenta manifestaciones digestivas persistentes incluyendo náusea, malestar epigástrico, distensión abdominal o cambios significativos en evacuaciones más allá de dos semanas de uso, considerar reducción de dosis, administración con alimentos más sustanciales, división de dosis en tomas espaciadas, o discontinuación temporal con reevaluación gradual.
- Discontinuar inmediatamente el uso si experimenta manifestaciones de hipersensibilidad incluyendo urticaria, prurito generalizado, hinchazón facial o labial, dificultad respiratoria o sibilancias que pueden indicar reacción alérgica requiriendo evaluación apropiada, aunque tales reacciones son raras con componentes en esta formulación.
- No exceder dosis total de seis a ocho cápsulas en periodo de veinticuatro horas independientemente de cantidad de alcohol consumida, para prevenir ingesta excesiva de componentes individuales particularmente vitaminas del complejo B donde aunque límites superiores tolerables son elevados, dosis muy elevadas sostenidas pueden generar manifestaciones.
- Evitar combinación de alcohol con estimulantes incluyendo cafeína en dosis elevadas o bebidas energéticas que enmascaran percepción de nivel de intoxicación mediante efectos estimulantes que contrarrestan efectos depresores de alcohol, permitiendo consumo excesivo sin reconocimiento apropiado de compromiso de función cognitiva y motora, independientemente de uso de suplementación.
- Evitar combinación de alcohol con sustancias depresoras del sistema nervioso central incluyendo sedantes, benzodiacepinas, opioides o antihistamínicos sedantes que potencian efectos depresores mediante mecanismos aditivos o sinérgicos incrementando riesgo de sedación excesiva o depresión respiratoria.
- Reconocer que esta fórmula no modifica concentración sanguínea de alcohol ni elimina efectos sobre función cognitiva, coordinación motora, tiempo de reacción o juicio que son críticos para conducción segura de vehículos, estableciendo que planificación de transporte alternativo es necesaria independientemente de suplementación cuando alcohol ha sido consumido.
- Asegurar hidratación apropiada mediante consumo de al menos dos a tres litros de agua distribuidos durante día cuando fórmula es utilizada, particularmente durante y después de consumo de alcohol dado que efectos diuréticos de alcohol generan deshidratación que contribuye significativamente a manifestaciones adversas y que hidratación optimiza excreción de metabolitos.
- Evitar uso de esta fórmula como justificación o facilitación de consumo incrementado de alcohol reconociendo que daño acumulativo de alcohol sobre hígado, cerebro, tracto gastrointestinal y otros órganos ocurre independientemente de efectividad de suplementación en modulación de manifestaciones agudas.
- Las personas con historial de consumo problemático de alcohol o dependencia deben reconocer que esta fórmula no es apropiada como intervención para estas condiciones que requieren aproximaciones especializadas, y que uso de suplemento diseñado para soporte durante consumo puede ser contraproducente en contexto de necesidad de abstinencia.
- Implementar ciclos de uso de ocho a doce semanas de administración diaria seguidos de pausas de siete a diez días cuando fórmula es utilizada como soporte metabólico hepático continuo en contexto de consumo regular de alcohol, permitiendo evaluación de efectos sostenidos y prevención de acumulación excesiva.
- Durante pausas de suplementación, mantener alimentación equilibrada rica en precursores de glutatión incluyendo proteínas que proporcionan aminoácidos azufrados, vegetales crucíferos que inducen expresión de enzimas de detoxificación, y fuentes dietéticas de vitaminas del complejo B para mantenimiento de homeostasis metabólica.
- Priorizar sueño de calidad apropiada de siete a nueve horas tras consumo de alcohol reconociendo que aunque alcohol puede facilitar inicio de sueño compromete arquitectura y calidad mediante supresión de sueño REM y fragmentación, y que recuperación completa requiere múltiples noches de sueño reparador.
- Evitar ejercicio intenso incluyendo entrenamiento de intervalos de alta intensidad o levantamiento de pesas pesadas durante veinticuatro a cuarenta y ocho horas después de consumo significativo de alcohol, limitando actividad a ejercicio ligero a moderado que promueve circulación sin generar estrés cardiovascular o metabólico excesivo.
- Documentar cantidad de alcohol consumida, timing de administración de suplemento, y respuesta percibida incluyendo intensidad y duración de manifestaciones que proporciona retroalimentación para optimización de protocolo individual mediante ajustes iterativos basados en experiencia acumulada.
- Si no observa modulación de manifestaciones tras tres a cuatro usos con adherencia apropiada a protocolo de dosificación preventiva y post-consumo, considerar que variabilidad individual en respuesta es sustancial reflejando polimorfismos genéticos y factores de estilo de vida, y que efectividad puede ser limitada en algunos individuos.
- Verificar composición de cápsulas en panel de ingredientes si sigue restricciones dietéticas específicas incluyendo alimentación vegetariana o vegana donde gelatina derivada de colágeno animal no es apropiada, mientras hidroxipropilmetilcelulosa que es polímero vegetal es compatible.
- Las personas que consumen múltiples suplementos regularmente incluyendo multivitamínicos que contienen vitaminas del complejo B, suplementos de minerales, o antioxidantes deben revisar composición total para prevenir duplicación excesiva de componentes y para evaluar necesidad de cada suplemento en protocolo integral.
- Mantener separación temporal de al menos dos horas entre este suplemento y suplementos de minerales en dosis elevadas particularmente calcio, magnesio o zinc para minimizar competencia por absorción mediante transportadores de metales divalentes compartidos en mucosa intestinal.
- Informar a profesionales de salud sobre suplementación con este producto antes de análisis de laboratorio que evalúan función hepática, niveles de vitaminas, o parámetros relacionados con metabolismo, permitiendo interpretación apropiada de resultados considerando influencia de suplementación.
- Si experimenta cambios no anticipados en energía, sueño, función digestiva o cualquier otro parámetro durante uso que genera preocupación, discontinuar temporalmente suplementación para evaluación de causalidad y considerar si modificaciones de protocolo o discontinuación permanente son apropiadas.
- No utilizar como única estrategia para minimización de efectos de alcohol; integrar suplementación con moderación consciente de cantidad y frecuencia de consumo, hidratación apropiada mediante alternancia de agua entre bebidas alcohólicas, consumo de alimentos antes y durante ingesta de alcohol, y priorización de sueño y recuperación.
- Los efectos percibidos pueden variar entre individuos; este producto complementa la dieta dentro de un estilo de vida equilibrado.
- Se desaconseja enfáticamente el uso durante embarazo dado que consumo de alcohol durante gestación está contraindicado por riesgo de efectos teratogénicos sobre desarrollo fetal incluyendo espectro de desórdenes fetales por alcohol que compromete desarrollo neurológico, facial y de múltiples órganos, estableciendo que suplemento diseñado para soporte durante consumo de alcohol es fundamentalmente inapropiado en esta población. Adicionalmente, la evidencia de seguridad de componentes específicos incluyendo dihidromiricetina durante embarazo es insuficiente con ausencia de estudios controlados en humanos que evalúen efectos sobre desarrollo fetal, organogénesis y función placentaria, mientras que aunque vitaminas del complejo B son nutrientes esenciales durante embarazo las dosis específicas en formulación suplemental combinadas con otros componentes no han sido evaluadas sistemáticamente en gestantes.
- Se desaconseja el uso durante lactancia dado que consumo de alcohol durante periodo de lactancia está desaconsejado porque etanol pasa a leche materna alcanzando concentraciones que aproximan concentración sanguínea materna y exposición de lactante puede comprometer desarrollo neurológico, alterar patrones de sueño y alimentación, y reducir producción de leche mediante inhibición de reflejo de eyección. La seguridad de componentes de fórmula incluyendo dihidromiricetina, NACET y extracto de jengibre durante lactancia no ha sido establecida mediante estudios que evalúen transferencia a leche materna, exposición neonatal resultante, o efectos sobre desarrollo de lactante, estableciendo que uso durante lactancia se desaconseja por insuficiente caracterización de seguridad en esta población vulnerable.
- Evitar el uso en personas con función hepática severamente comprometida incluyendo insuficiencia hepática descompensada, cirrosis avanzada con hipertensión portal o ascitis, o falla hepática aguda, dado que metabolismo de componentes de fórmula incluyendo conjugación de dihidromiricetina con ácido glucurónico, hidrólisis y metabolismo de NACET, y fosforilación de vitaminas del complejo B ocurre predominantemente en hígado y función hepática severamente comprometida puede generar acumulación de componentes o metabolitos. Fundamentalmente, consumo de alcohol en contexto de enfermedad hepática establecida es contraindicado independientemente de suplementación dado que alcohol exacerba daño hepático, compromete regeneración y acelera progresión de enfermedad, estableciendo que uso de suplemento diseñado para soporte durante consumo de alcohol es inapropiado en esta población donde abstinencia completa es recomendación fundamental.
- Se desaconseja el uso concomitante con anticoagulantes incluyendo warfarina, acenocumarol, o anticoagulantes orales directos incluyendo dabigatrán, rivaroxabán y apixabán sin evaluación apropiada, dado que extracto de jengibre contiene gingeroles que inhiben ciclooxigenasa reduciendo síntesis de tromboxano A2 que promueve agregación plaquetaria, y que pueden modular coagulación mediante mecanismos adicionales aunque evidencia de interacciones clínicamente significativas con dosis suplementales de jengibre es limitada y predominantemente teórica. La combinación de alcohol con anticoagulantes incrementa independientemente riesgo de sangrado mediante efectos sobre función plaquetaria y metabolismo de factores de coagulación, estableciendo precaución adicional cuando alcohol es consumido por individuos en terapia anticoagulante independientemente de suplementación.
- Evitar el uso en personas que consumen disulfiram que es fármaco utilizado como disuasivo de consumo de alcohol mediante inhibición de aldehído deshidrogenasa que genera acumulación severa de acetaldehído cuando alcohol es consumido, produciendo manifestaciones aversivas intensas incluyendo rubor facial, taquicardia, hipotensión y náusea severa. Aunque esta fórmula contiene componentes que favorecen actividad de aldehído deshigrogenasa y conjugación de acetaldehído, la inhibición farmacológica por disulfiram es potente y no es contrarrestada significativamente por suplementación, estableciendo que individuos en tratamiento con disulfiram no deben consumir alcohol independientemente de uso de suplementos, y que uso de fórmula diseñada para soporte durante consumo de alcohol es contradictorio con objetivo terapéutico de disuasión de consumo.
- Se desaconseja el uso en personas con historial documentado de hipersensibilidad severa o reacciones anafilácticas a plantas de familia Zingiberaceae que incluye jengibre, cúrcuma y cardamomo, dado que extracto de jengibre es componente de formulación y exposición puede desencadenar reacción de hipersensibilidad tipo I mediada por IgE que puede manifestarse como urticaria, angioedema, broncoespasmo o en casos severos shock anafiláctico. Adicionalmente, evitar el uso en personas con hipersensibilidad conocida a Hovenia dulcis que es fuente de dihidromiricetina, o a excipientes de cápsulas incluyendo gelatina derivada de colágeno que puede causar reacciones en individuos con alergia a proteínas animales específicas.
- Evitar el uso en personas que consumen inhibidores de monoamino oxidasa incluyendo fenelzina, tranilcipromina o selegilina en dosis no selectivas, dado que tiramina que puede estar presente en pequeñas cantidades en extractos herbales o que puede ser formada durante metabolismo de aminoácidos puede desencadenar crisis hipertensiva en presencia de inhibición de MAO que previene degradación de tiramina. Adicionalmente, consumo de alcohol en combinación con inhibidores de MAO puede generar interacciones complejas incluyendo potenciación de efectos depresores sobre sistema nervioso central y modulación de metabolismo de neurotransmisores, estableciendo que combinación requiere precaución extrema independientemente de suplementación.
- Se desaconseja el uso en personas con trastornos de coagulación incluyendo hemofilia, enfermedad de von Willebrand, o trombocitopenia severa, dado que extracto de jengibre puede modular función plaquetaria mediante inhibición de síntesis de tromboxano y que alcohol también compromete hemostasia mediante múltiples mecanismos incluyendo efectos sobre síntesis hepática de factores de coagulación y función plaquetaria. La combinación de múltiples factores que comprometen coagulación puede incrementar riesgo de sangrado particularmente cuando trauma o procedimientos quirúrgicos ocurren, estableciendo que individuos con trastornos de coagulación deben evitar tanto consumo de alcohol como suplementación con componentes que modulan hemostasia.
- Evitar el uso en personas programadas para cirugía electiva durante periodo de dos semanas previas a procedimiento, dado que extracto de jengibre puede modular agregación plaquetaria y hemostasia incrementando riesgo de sangrado perioperatorio, y dado que metabolismo de anestésicos y otros fármacos utilizados durante cirugía puede ser modulado por componentes de fórmula mediante efectos sobre citocromos P450. Adicionalmente, consumo de alcohol debe ser descontinuado durante periodo preoperatorio para optimización de función hepática, reducción de riesgo de complicaciones anestésicas, y facilitación de cicatrización postoperatoria, estableciendo que uso de fórmula diseñada para soporte durante consumo de alcohol es inapropiado durante periodo perioperatorio.
- Se desaconseja el uso en personas con úlcera péptica activa o sangrado gastrointestinal agudo, dado que extracto de jengibre puede incrementar secreción gástrica y modular motilidad de manera que puede exacerbar manifestaciones, y dado que alcohol es irritante directo de mucosa gástrica que compromete integridad de barrera mucosa, incrementa secreción ácida y reduce producción de prostaglandinas protectoras. La combinación de consumo de alcohol con úlcera péptica activa incrementa significativamente riesgo de sangrado y perforación independientemente de suplementación, estableciendo que abstinencia de alcohol es recomendación fundamental durante periodo de curación de úlcera.
- Evitar el uso en personas con cálculos biliares o obstrucción del ducto biliar, dado que componentes incluyendo extracto de jengibre pueden estimular contracción de vesícula biliar y flujo biliar que en presencia de obstrucción puede generar cólico biliar severo o en casos extremos colecistitis. El NACET y otros componentes lipofílicos requieren emulsificación por sales biliares para absorción apropiada estableciendo demanda incrementada de función biliar, y compromiso de flujo biliar puede alterar farmacocinética de componentes reduciendo absorción.
- Se desaconseja el uso en personas con hipoglucemia recurrente o que utilizan medicación antidiabética incluyendo insulina o sulfonilureas, dado que consumo de alcohol inhibe gluconeogénesis hepática mediante generación de NADH elevado que favorece conversión de piruvato a lactato más que oxidación a acetil-CoA, predisponiendo a hipoglucemia particularmente cuando consumo ocurre sin ingesta adecuada de carbohidratos. Aunque esta fórmula contiene cofactores que participan en metabolismo de carbohidratos, no previene hipoglucemia inducida por alcohol estableciendo que individuos con riesgo de hipoglucemia deben moderar consumo de alcohol extremadamente, monitorizar glucemia apropiadamente, y asegurar consumo de carbohidratos antes y durante ingesta de alcohol independientemente de suplementación.
Let customers speak for us
from 145 reviewsYa voy por mi segunda compra de Azul de Metileno al 1%, excelente producto. En mi caso puedo asegurar que el efecto es idéntico a la descripción que brindan del mismo aquí en la página web. Gracias!

El precio es muy bueno si la tubiera que comparar con otras marcas, la calidad del producto tam bién eh visto mejoras en mi organismo.

Se siente el resultado en poco tiempo. Mi ciclo del sueño se ha reprogramafo y logro dormirme en poco tiempo y profundamente lo que me permite amanecer con más energía y ánimo.

una buena experiencia los productos son de muy buena calidad, deberian hacer promociones para clientes
muy bueno

excelente producto ayuda a conciliar el sueño

buenisimo


excelente producto




muy bueno y sludable

Todo perfecto, a tiempo y con calidez para la atención
Tengo 5 semanas usando RATRITUTRIDA y es simplemente MARAVILLOSO, me quito la ansiedad, el hambre está MUY CONTROLADO, tengo energía ya que estoy siguiendo TODO el protocolo para pérdida de grasa. Lo estoy probando en mi porque mi producto NUTRIHIPNOSIS llevará el protocolo y si en mi funciona también lo hará en mis pacientes. MARAVILLADA

Este producto funciona de manera efectiva, yo lo tomo un rato después de la última bebida, creeme que afectará de manera positiva la forma en como te sientes al día siguiente. En resumidas cuentas, esta fórmula trabaja activamente para descomponer y eliminar el acetaldehído del cuerpo, te sentirás mejor después de una noche de tragos, gran creación, gracias

Nada de resaca como lo prometen, me pareció increíble
⚖️ DISCLAIMER / DESCARGO DE RESPONSABILIDAD
La información presentada en esta página tiene fines exclusivamente educativos, informativos y de orientación general sobre nutrición, bienestar y biooptimización.
Los productos mencionados no están destinados a diagnosticar, tratar, curar ni prevenir ninguna enfermedad, y no deben considerarse como sustitutos de una evaluación médica profesional ni del consejo de un profesional de la salud calificado.
Los protocolos, combinaciones y recomendaciones descritas se basan en investigaciones científicas publicadas, literatura nutricional internacional y experiencias de usuarios o profesionales del ámbito del bienestar, pero no constituyen una prescripción médica. Cada organismo es diferente, por lo que la respuesta a los suplementos puede variar según factores individuales como la edad, el estilo de vida, la alimentación, el metabolismo y el estado fisiológico general.
Nootrópicos Perú actúa únicamente como proveedor de suplementos nutricionales y compuestos de investigación de libre comercialización en el país, los cuales cumplen con estándares internacionales de pureza y calidad. Los productos son comercializados para uso complementario, dentro de un estilo de vida saludable y bajo responsabilidad del consumidor.
Antes de iniciar cualquier protocolo o incorporar nuevos suplementos, se recomienda consultar a un profesional de la salud o nutrición para determinar la conveniencia y dosis adecuada en cada caso.
El uso de la información contenida en este sitio es de responsabilidad exclusiva del usuario.
De acuerdo con la normativa vigente del Ministerio de Salud y DIGESA, todos los productos se ofrecen como suplementos alimenticios o compuestos nutricionales de libre venta, sin carácter farmacológico o medicinal. Las descripciones incluidas hacen referencia a su composición, origen y posibles funciones fisiológicas, sin atribuir propiedades terapéuticas, preventivas o curativas.